A diagnosis of coronary artery blockage often makes patients assume that a permanent metal stent will always be required. While drug-eluting stents remain an important and widely used treatment for coronary artery disease, selected blockages can now be treated using a minimally invasive technique known as stentless angioplasty with a Drug-Eluting Balloon, or DEB.
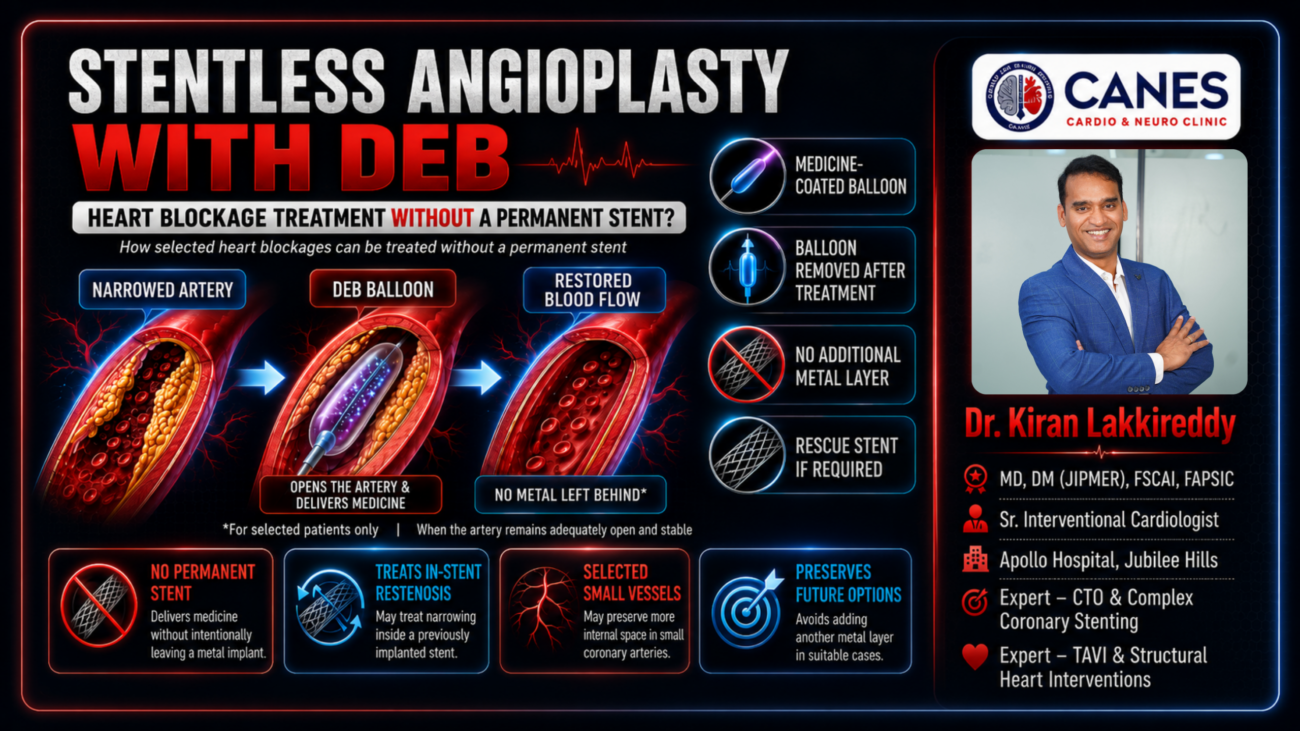
A Drug-Eluting Balloon is a special angioplasty balloon coated with medicine. It is guided into the narrowed section of the coronary artery, inflated for a controlled period and then removed from the body. During inflation, the medicine is transferred directly to the artery wall, helping reduce excessive tissue growth and the chance of the artery narrowing again.
When the treated artery remains adequately open and stable, no permanent metal stent needs to be left behind.
At CANES Cardio and Neuro Clinic in Hyderabad, Dr. Kiran Lakkireddy evaluates patients with coronary artery disease to determine whether they may benefit from DEB angioplasty, drug-eluting stent placement, bypass surgery or medical treatment.
Quick Answer
Stentless angioplasty with DEB is a minimally invasive procedure that treats selected coronary artery blockages without intentionally leaving a permanent stent inside the artery.
During the procedure, the cardiologist first opens and prepares the narrowed section using standard or specialised angioplasty balloons. A Drug-Eluting Balloon is then positioned across the treated area and inflated. The medicine on the balloon is transferred to the artery wall, after which the balloon is deflated and removed.
The treatment can be especially useful for selected patients with narrowing inside a previously implanted stent, small coronary arteries or situations where adding another layer of metal may not be desirable.
However, a DEB-only approach is not suitable for every blockage. If the artery does not remain open, shows severe recoil or develops a major tear that affects blood flow, a drug-eluting stent may still be required.
What Is a Drug-Eluting Balloon?
A Drug-Eluting Balloon is a catheter-mounted angioplasty balloon coated with medicine that helps control excessive tissue growth inside the artery. It is also commonly called a Drug-Coated Balloon or DCB.
The balloon does not stay permanently inside the heart. It remains in the narrowed section only long enough to open the artery and transfer the medicine to the vessel wall.
After the medicine has been delivered, the balloon and catheter are completely removed.
This makes DEB angioplasty different from conventional stent angioplasty. A stent is a small metallic mesh tube that remains permanently inside the artery to provide structural support. A Drug-Eluting Balloon delivers medicine but does not leave a permanent framework behind.
What Does Stentless Angioplasty Mean?
Stentless angioplasty means that the cardiologist plans to treat the coronary blockage without placing a permanent metal stent.
The term does not mean that a stent can never be used during the procedure. A stentless strategy is successful only when the artery opens adequately and remains stable after balloon treatment.
Before completing the procedure without a stent, the cardiologist confirms that blood flow is satisfactory, the remaining narrowing is acceptable and there is no major dissection or vessel collapse.
If the artery does not remain safely open, the cardiologist may place a drug-eluting stent. This is called rescue stenting or bailout stenting.
Rescue stenting is not considered a failure. It is a safety measure used when the vessel requires permanent support.
How Is DEB Angioplasty Different From Stent Angioplasty?
Both DEB angioplasty and stent angioplasty are used to restore blood flow through narrowed coronary arteries. The main difference is whether a permanent implant remains inside the artery.
During drug-eluting stent angioplasty, the blockage is expanded and a metal mesh stent is implanted. The stent supports the vessel wall and releases medicine over time. It remains permanently inside the artery.
During DEB angioplasty, the artery is prepared using balloons or other equipment. The Drug-Eluting Balloon is then inflated to transfer medicine to the vessel wall and is removed afterward.
A stent provides both medicine and mechanical support. A DEB mainly delivers medicine. Therefore, a DEB-only approach can be used only when the artery remains open without a permanent scaffold.
Why Is Proper Artery Preparation Important?
Preparing the artery correctly is one of the most important parts of DEB angioplasty.
Because no permanent stent is left behind, the narrowed segment must be expanded effectively before the Drug-Eluting Balloon is used. Poor preparation can prevent the medicine from reaching the artery wall evenly and may leave the vessel inadequately opened.
Depending on the nature of the blockage, the cardiologist may use a standard balloon, high-pressure balloon, non-compliant balloon, scoring balloon or cutting balloon.
Calcified blockages may require specialised calcium-modification techniques before DEB treatment can be considered.
Intravascular imaging such as IVUS or OCT may also be used to examine the blockage from inside the artery. These technologies help the cardiologist identify calcium, plaque, an underexpanded previous stent, tissue growth or other mechanical problems.
Proper preparation helps determine whether the artery is likely to remain stable without a stent.
Who May Benefit From Stentless Angioplasty With DEB?
DEB angioplasty is not selected simply because a patient wishes to avoid a stent. It is recommended only when the lesion anatomy and final balloon result make a stentless approach safe and appropriate.
DEB for In-Stent Restenosis
In-stent restenosis occurs when a previously treated artery becomes narrow again inside or near an existing stent.
This may happen because of excessive tissue growth, new plaque formation, inadequate expansion of the original stent, heavy calcium, stent fracture or multiple layers of overlapping metal.
A Drug-Eluting Balloon can deliver medicine inside the narrowed stent without necessarily adding another metal layer.
This can be particularly useful when the artery already contains one or more stents. Placing an additional stent may reduce the space available for blood flow and make future treatment more difficult.
However, the underlying reason for the restenosis must first be identified. If the original stent is severely underexpanded, simply using a Drug-Eluting Balloon may not provide a lasting result. The mechanical problem must be corrected before medicine is delivered.
DEB for Small Coronary Arteries
Small coronary arteries can be challenging to treat because even a thin metallic stent occupies some space inside the vessel.
In selected small-vessel blockages, a DEB strategy may help preserve the natural internal diameter of the artery and avoid leaving permanent metal behind.
The artery must still be carefully prepared and must remain open after balloon treatment. A DEB should not be used in a small vessel when the final result is unstable or inadequate.
DEB for Bifurcation Blockages
A bifurcation blockage occurs where one coronary artery divides into two branches.
Treating both branches with stents can sometimes create overlapping metal or make access to the smaller branch more difficult. In selected cases, the cardiologist may place a stent in the main branch and use a Drug-Eluting Balloon in the side branch.
A DEB-only strategy may also be considered in specific bifurcation anatomies.
The treatment depends on the size, angle and importance of each branch. Bifurcation procedures require careful planning and should be individualised.
DEB for Patients With Multiple Existing Stents
Some patients have more than one stent layer in the same section of an artery.
Adding another stent can make the artery increasingly rigid, reduce the internal space and complicate future procedures.
A Drug-Eluting Balloon may allow medicine to be delivered without adding another permanent metal layer. Before using a DEB, the cardiologist must check the existing stents for underexpansion, fracture, distortion, calcium or new tissue growth.
DEB for Patients With Increased Bleeding Risk
Patients undergoing coronary angioplasty usually need antiplatelet medicines to reduce the risk of blood-clot formation.
In selected patients treated successfully with a DEB-only strategy, the cardiologist may consider a different or sometimes shorter antiplatelet plan than would be required after complex stent implantation.
However, this varies from patient to patient. The duration depends on whether a rescue stent was placed, whether the patient had a heart attack, previous stent history, bleeding risk and other medical conditions.
Patients must never stop aspirin, clopidogrel, ticagrelor or any other prescribed antiplatelet medicine without consulting their cardiologist.
Can DEB Be Used for a New Coronary Blockage?
A previously untreated coronary blockage is known as a new or de novo lesion.
DEB angioplasty may be considered for selected new blockages, particularly in certain small coronary arteries. However, modern drug-eluting stents remain the preferred treatment for many new coronary lesions.
A stentless strategy may be considered only when the blockage can be prepared properly, blood flow is fully restored and the artery remains stable without major recoil or dissection.
The choice should be based on the artery, lesion type and expected long-term result rather than on avoiding a stent at any cost.
Who May Not Be Suitable for DEB Angioplasty?
A DEB-only strategy may not be suitable when the coronary artery requires permanent structural support.
This may include blockages with severe recoil, heavy calcium that prevents proper expansion, major vessel dissection, inadequate blood flow, a large amount of residual narrowing or sudden artery closure.
Very long or highly complex lesions may also be better treated with a drug-eluting stent or bypass surgery.
A DEB-only approach may also be inappropriate when the patient cannot take the required antiplatelet medicines or when the cardiologist believes another treatment will provide a safer and more durable result.
The purpose of DEB angioplasty is not simply to avoid metal. The goal is to restore reliable blood flow using the most appropriate treatment.
What Tests Are Required Before DEB Angioplasty?
The cardiologist may recommend several investigations before deciding whether DEB angioplasty is appropriate.
An electrocardiogram records the electrical activity of the heart and may identify reduced blood supply, previous heart damage or rhythm disturbances.
An echocardiogram evaluates the pumping strength of the heart, heart chamber size, valves and areas of weak heart muscle.
Blood investigations may be performed to assess haemoglobin, kidney function, blood sugar, cholesterol, clotting and cardiac enzymes.
A treadmill test, stress echocardiogram or nuclear perfusion scan may be recommended to determine whether a coronary narrowing is reducing blood supply during activity.
CT coronary angiography may provide a non-invasive view of the coronary arteries in selected patients.
Coronary angiography remains the main investigation used to identify the exact location, length and severity of the blockage. It also helps the cardiologist decide whether the patient should receive medical treatment, DEB angioplasty, stenting or bypass surgery.
Pressure-based tests such as FFR or iFR may be used to determine whether an intermediate blockage is significantly reducing blood flow.
Intravascular imaging with IVUS or OCT may be especially useful when treating narrowing inside a previous stent. It can reveal stent underexpansion, fracture, calcium, tissue growth or new plaque formation.
How Is Stentless Angioplasty With DEB Performed?
The procedure is performed in a cardiac catheterisation laboratory.
Local anaesthesia is usually given at the wrist or groin. Mild sedation may also be provided to help the patient remain comfortable.
A small tube called a sheath is inserted into the artery. A guiding catheter is then advanced toward the opening of the coronary artery.
Contrast dye is injected so that the blockage can be seen under X-ray guidance.
A very thin guidewire is passed across the narrowed section. This wire acts as a pathway for the balloons and other treatment equipment.
The cardiologist then evaluates the length of the blockage, artery size, calcium burden, existing stents, blood flow and the involvement of side branches.
The narrowed segment is carefully prepared using one or more balloons. Specialised balloons or calcium-modification techniques may be required for resistant lesions.
After preparation, the cardiologist checks whether the artery has opened adequately and whether it can remain stable without a stent.
If the result is satisfactory, the correctly sized Drug-Eluting Balloon is placed across the treated segment and inflated for a controlled period. This allows the medicine to transfer to the vessel wall.
The balloon is then deflated and removed.
A final angiogram is performed to confirm normal blood flow, acceptable remaining narrowing and the absence of major recoil or a flow-limiting dissection.
When Is Rescue Stenting Required?
A drug-eluting stent may be required when the artery does not remain safely open after balloon treatment.
Rescue stenting may be performed if the vessel begins to collapse, severe recoil develops, a major tear reduces blood flow or the blockage remains inadequately expanded.
It may also be required if the patient develops continuing chest pain or if the final angiographic result is not expected to remain stable.
The cardiologist’s first priority is safe and reliable blood flow. Therefore, the decision to place a rescue stent is based on patient safety rather than the original intention to perform a stentless procedure.
Benefits of Stentless Angioplasty With DEB
The main advantage of DEB angioplasty is that it can deliver medicine without leaving an additional permanent metal implant.
This may be helpful for patients with in-stent restenosis, small coronary vessels or multiple existing stents.
Avoiding another metal layer may preserve more internal space inside the artery and make future procedures less complex.
The treated artery may also retain more of its natural movement because it is not caged by a newly implanted stent.
A successful DEB-only procedure also avoids creating a new metallic surface on which stent thrombosis could occur. However, patients still have coronary artery disease and must continue all recommended medicines and lifestyle changes.
In selected patients, the antiplatelet treatment plan may also be different from that used after complex stent implantation. This decision must always be made by the treating cardiologist.
Possible Risks of DEB Angioplasty
DEB angioplasty is minimally invasive, but it still carries potential risks.
These may include bleeding or swelling at the wrist or groin, blood-vessel injury, allergic reaction to contrast dye, temporary kidney injury, abnormal heart rhythms, coronary artery dissection, vessel recoil or sudden artery closure.
Some patients may require emergency stent placement if the artery does not remain stable.
Rare complications can include heart attack, stroke, emergency bypass surgery or death.
The overall risk depends on the patient’s age, kidney function, heart function, diabetes, blockage complexity and previous heart procedures.
Is DEB Better Than a Drug-Eluting Stent?
Neither treatment is better for every patient.
A drug-eluting stent may be preferable when the artery requires permanent support, significant recoil is expected, the blockage is long or complex or the final balloon result is not satisfactory.
A DEB may be considered when a previous stent has narrowed again, the artery is small, adding another metal layer is undesirable or the vessel remains stable after careful preparation.
DEB and drug-eluting stents are different tools. The right treatment depends on the type of blockage and the result that can be achieved safely.
What Is In-Stent Restenosis?
In-stent restenosis is the re-narrowing of a coronary artery inside or close to a previously implanted stent.
Patients may experience recurring chest pain, breathlessness, reduced exercise capacity or fatigue. Some cases may be detected through an abnormal stress test, while others may present as an acute coronary syndrome.
Restenosis usually develops gradually because of tissue growth, new plaque formation, stent underexpansion, fracture or heavy calcium.
It is different from stent thrombosis, which is a sudden blood clot forming inside a stent. Stent thrombosis can cause an acute heart attack and requires emergency treatment.
Recovery After DEB Angioplasty
Recovery after an uncomplicated DEB procedure is often similar to recovery after conventional coronary angioplasty.
The medical team monitors the patient’s heart rate, blood pressure, rhythm, chest discomfort and the catheter-entry site.
Patients treated through the wrist may be able to sit up and walk relatively early.
Some patients may go home on the same day or the following day. A longer hospital stay may be needed after a heart attack, complex procedure, kidney problem, abnormal heart rhythm or rescue stent placement.
Mild bruising or discomfort at the wrist or groin may occur and usually improves gradually.
Care After Returning Home
Patients should take every prescribed medicine regularly and should never stop antiplatelet treatment without medical advice.
The wrist or groin entry site should be kept clean, and heavy lifting should be avoided for the period recommended by the cardiologist.
Blood pressure, diabetes and cholesterol should be controlled carefully. Smoking should be stopped, and a heart-healthy diet should be followed.
Cardiac rehabilitation may be recommended to help patients return safely to exercise and daily activity.
Recurring chest pain, sudden breathlessness, fainting, heavy bleeding or rapidly increasing swelling at the catheter site should be reported immediately.
A successful DEB procedure treats a particular narrowed segment. It does not cure the underlying tendency to develop coronary artery disease.
Medicines After DEB Angioplasty
Medicines after the procedure may include aspirin, clopidogrel, ticagrelor or another antiplatelet medicine.
Patients may also receive cholesterol-lowering statins, blood-pressure medicines, diabetes treatment, beta blockers or anti-anginal medicines.
The exact combination and duration depend on whether DEB alone was used, whether a rescue stent was placed, whether the procedure followed a heart attack and the patient’s bleeding risk.
Patients must follow the prescription provided by their cardiologist and should not change the dose or stop medication independently.
Common Myths About Stentless Angioplasty
Myth: DEB Can Replace Stents in Every Patient
Medical Fact: Many coronary blockages still require a drug-eluting stent for safe and durable support.
Myth: A Drug-Eluting Balloon Dissolves the Blockage
Medical Fact: The balloon expands the narrowed section and delivers medicine. It does not dissolve or remove all plaque from the artery.
Myth: No Stent Means No Medicines Are Needed
Medical Fact: Antiplatelet medicines, statins and other heart treatments may still be required after DEB angioplasty.
Myth: DEB Is the Same as Normal Balloon Angioplasty
Medical Fact: A Drug-Eluting Balloon carries medicine that helps reduce excessive tissue growth and repeated narrowing.
Myth: Rescue Stenting Means the Procedure Has Failed
Medical Fact: Rescue stenting is an important safety measure used when the artery requires permanent support.
Myth: DEB Always Provides Better Results Than a Stent
Medical Fact: The best treatment depends on the type of blockage, artery size, vessel stability and the underlying reason for the narrowing.
Myth: Stentless Angioplasty Permanently Cures Coronary Disease
Medical Fact: The procedure treats a specific blockage. Long-term medicines and lifestyle changes remain essential.
Stentless Angioplasty With DEB at CANES Clinic
Successful DEB angioplasty requires an accurate diagnosis, detailed angiogram assessment, proper lesion preparation, correct balloon sizing and careful evaluation of the final blood flow.
At CANES Cardio and Neuro Clinic in Hyderabad, patients with coronary artery disease are evaluated under the guidance of Dr. Kiran Lakkireddy, an experienced interventional cardiologist.
Each patient is assessed individually to determine whether the blockage is new or located inside a previous stent, whether multiple stent layers are already present, whether significant calcium exists and whether the artery is likely to remain stable after balloon preparation.
The purpose is not simply to avoid a stent. The goal is to restore reliable coronary blood flow using the safest and most appropriate treatment for the patient.
● Location: 3rd Floor, Tapasavi Commercial Complex, Hi-Tension Rd, Kondapur, Hyderabad
● Contact: +91 9014944654
● Appointment Booking: Visit the CANES Clinic Official Portal
● Specialist Profile: Dr. Kiran Lakkireddy Official Website
Frequently Asked Questions
What Is the Full Form of DEB?
DEB stands for Drug-Eluting Balloon. It is also commonly called a Drug-Coated Balloon or DCB.
Does the Drug-Eluting Balloon Remain Inside the Body?
No. The balloon delivers medicine to the artery wall and is then deflated and removed.
Is DEB Angioplasty Completely Stent-Free?
It can be completed without a stent when the artery remains adequately open and stable. A rescue stent may still be required if severe recoil, inadequate expansion or a major dissection occurs.
Can DEB Treat a Blockage Inside an Old Stent?
Yes. In-stent restenosis is one of the main situations in which DEB angioplasty may be considered. The reason for the previous stent narrowing should be identified before treatment.
Can DEB Be Used for a New Coronary Blockage?
It may be used for selected new blockages, particularly in certain small coronary arteries. It is not suitable for every new lesion.
Is DEB Better Than a Drug-Eluting Stent?
Not in every case. A DEB may be suitable when another metal layer is undesirable, while a stent may be better when the artery needs permanent structural support.
Does DEB Remove All the Plaque?
No. The balloon expands the artery and delivers medicine. It does not remove all the plaque from the vessel wall.
Is General Anaesthesia Required?
Usually not. DEB angioplasty is generally performed under local anaesthesia at the wrist or groin. Mild sedation may also be given.
How Long Does the Procedure Take?
The procedure time depends on the number, location and complexity of the blockages. Treating heavy calcium or narrowing inside an old stent may take longer.
How Long Will I Stay in the Hospital?
Some patients may go home on the same day or the following day. A longer stay may be required after a heart attack or complex intervention.
Will I Need Blood-Thinning Medicines?
Yes. Antiplatelet medication is generally required after DEB angioplasty. The exact medicine and duration depend on the procedure and the patient’s overall condition.
Can the Artery Become Narrow Again?
Yes. The medicine on the balloon reduces excessive tissue growth, but no treatment can completely eliminate the possibility of restenosis.
Can DEB Be Used Inside Multiple Stents?
It may be considered to avoid adding another metal layer. The existing stents must first be evaluated for underexpansion, fracture and calcium.
Is DEB Suitable for a Calcified Blockage?
Selected calcified blockages may be suitable after effective calcium modification. If the artery cannot be expanded properly, a DEB-only strategy may not be safe.
When Can Normal Activities Be Resumed?
Light activity may often be resumed relatively early. Heavy lifting and strenuous exercise should be avoided until approved by the cardiologist.
Which Symptoms Need Urgent Medical Attention?
Urgent medical care should be sought for severe or persistent chest pain, sudden breathlessness, fainting, heavy bleeding from the wrist or groin, rapidly increasing swelling, new weakness or difficulty speaking