Left Heart Failure: A Complete Guide to Symptoms, Diagnosis, Treatment and Long-Term Heart Care
Table of Contents
- Introduction
- What Is Left Heart Failure?
- Is Left Heart Failure the Same as Congestive Heart Failure?
- What Are the Main Types of Left Heart Failure?
- Acute Versus Chronic Left Heart Failure
- What Causes Left Heart Failure?
- What Are the Symptoms of Left Heart Failure?
- Which Symptoms Require Emergency Medical Care?
- How Is Left Heart Failure Diagnosed?
- How Is Left Heart Failure Treated?
- Medicines for Left Heart Failure
- Does Treatment Differ According to Ejection Fraction?
- Actionable Checklist: What Should Patients Ask Their Cardiac-Care Team?
- Cardiovascular Guidance at CANES Clinic
- FAQs
Book a Consultation
Prevention is better than cure. Talk to our specialists today.
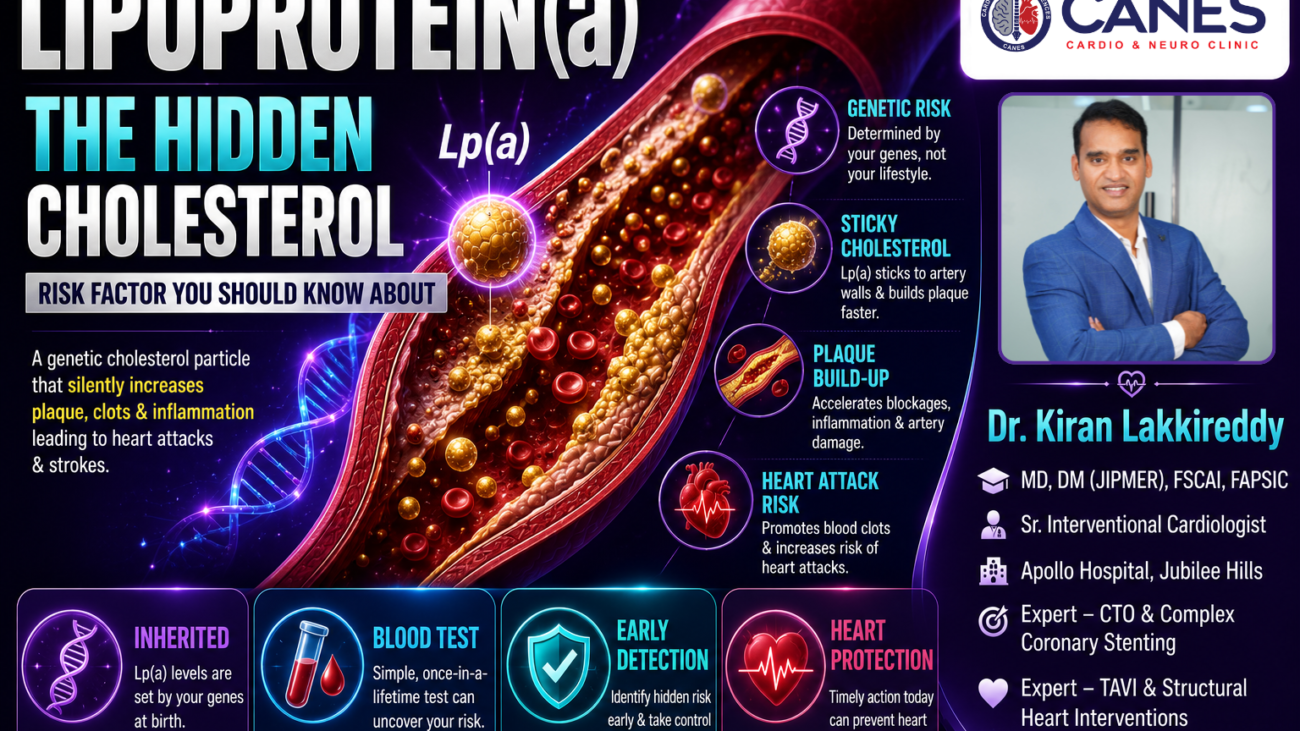
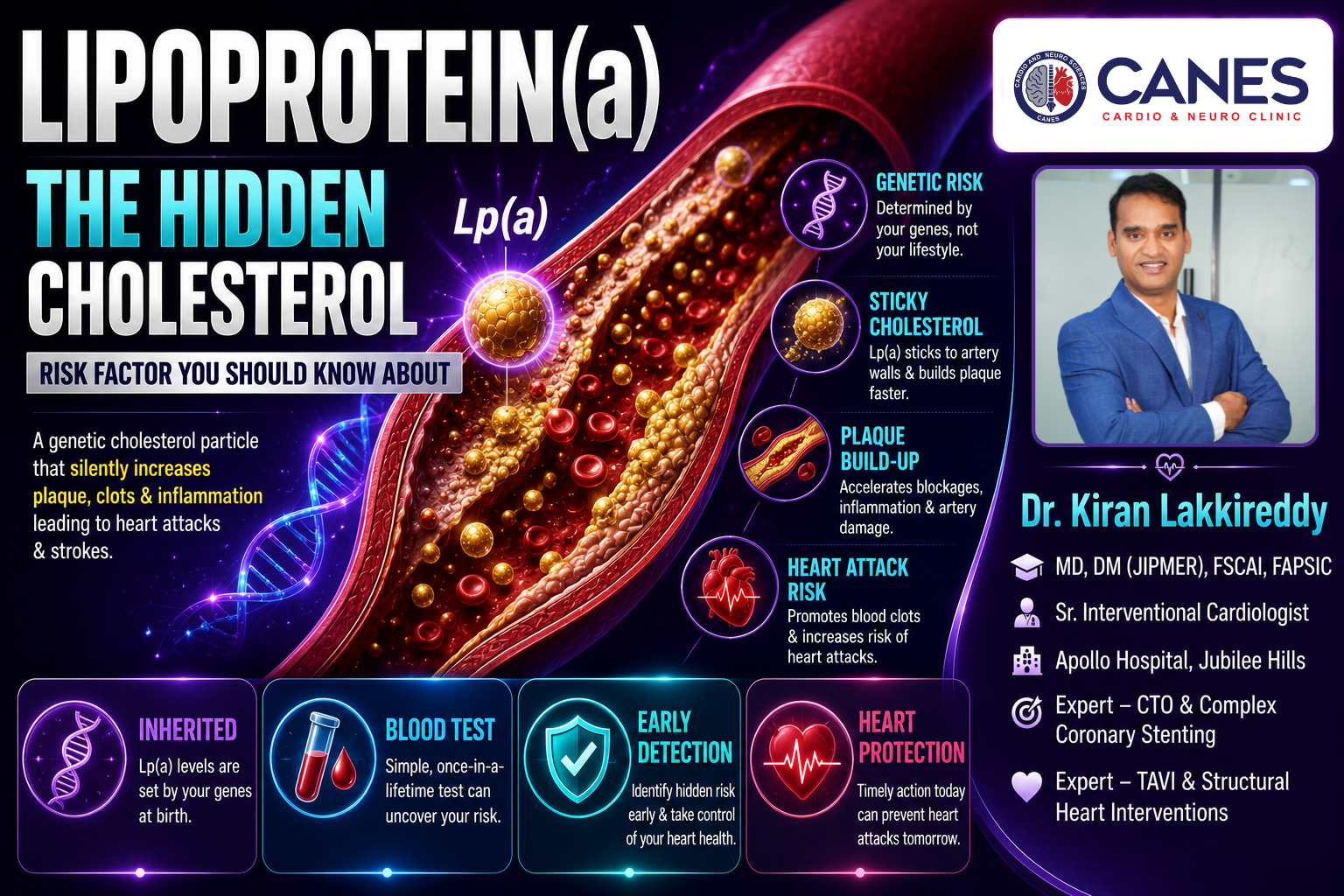
The left side of the heart performs most of the work required to deliver oxygen-rich blood throughout the body. Blood returning from the lungs enters the left atrium and then moves into the left ventricle, which pumps it through the aorta to the body’s organs and tissues.
Left heart failure, also known as left-sided or left ventricular heart failure, develops when the left side of the heart cannot pump or fill effectively enough to meet the body’s needs. This does not mean that the heart has stopped. It means that its pumping or filling function has become impaired.
When the left ventricle cannot move blood forward efficiently, pressure may build up behind it in the left atrium and the blood vessels of the lungs. This can cause breathlessness, coughing and fluid accumulation in the lungs. Reduced blood flow to the body may also contribute to fatigue, weakness and reduced exercise capacity. Left heart failure is not a single disease. It is a clinical condition that can result from coronary artery disease, a previous heart attack, high blood pressure, cardiomyopathy, heart-valve disease, abnormal heart rhythms and several other conditions.
Treatment depends on the underlying cause, the patient’s symptoms, the heart’s ejection fraction, kidney function, blood pressure, heart rhythm and other medical conditions. Management may involve medicines, lifestyle changes, cardiac rehabilitation, treatment of blocked arteries or diseased valves, implanted devices or advanced heart-failure therapies.
At CANES Cardio & Neuro Clinic, a specialised cardiovascular care centre in Hyderabad, the approach emphasises detailed cardiovascular assessment, understandable patient education and shared decision-making. Guided by Dr. Kiran Lakkireddy, an experienced interventional cardiologist specialising in complex cardiology, the clinic helps patients and families understand heart conditions, available treatment options and the importance of appropriate follow-up care.
Quick Answer
Left heart failure occurs when the left side of the heart cannot pump blood effectively or cannot relax and fill normally, leading to fluid backup in the lungs and reduced oxygen delivery to the body.
It may lead to:
- Shortness of breath during activity
- Difficulty breathing while lying flat
- Waking at night feeling breathless
- Persistent coughing or wheezing
- Fatigue and weakness
- Reduced exercise capacity
- Rapid or irregular heartbeat
- Fluid accumulation in the lungs
- Swelling and sudden weight gain when fluid retention becomes more extensive
Left heart failure may occur with a reduced, mildly reduced or preserved ejection fraction. An echocardiogram is commonly used to measure ejection fraction and assess the heart’s structure and function. Treatment options generally include:
- Medicines to reduce congestion
- Medicines that protect the heart and reduce its workload
- Blood-pressure, diabetes and cholesterol management
- Treatment of coronary artery disease
- Treatment of heart-valve disease
- Control of abnormal heart rhythms
- Medically guided physical activity
- Cardiac rehabilitation
- Implantable devices for selected patients
- Advanced therapies for severe heart failure
The correct treatment plan is individualised. Patients should not start, stop or change heart medicines without guidance from their treating healthcare professional.
Left Heart Failure at a Glance
Aspect | What It Means | Why It Matters |
|---|---|---|
Left ventricular dysfunction | The left ventricle cannot pump or fill normally | Can reduce blood flow to the body and increase pressure in the lungs |
Pulmonary congestion | Fluid and pressure build up in the lung circulation | Causes breathlessness, coughing and difficulty lying flat |
Reduced ejection fraction | The heart pumps out a smaller proportion of the blood it contains | Helps guide diagnosis and treatment |
Preserved ejection fraction | Pumping percentage remains preserved, but the ventricle may be stiff and fill abnormally | Symptoms can still be significant despite a normal-looking ejection fraction |
Acute heart failure | Symptoms appear suddenly or worsen rapidly | May require emergency hospital treatment |
Chronic heart failure | The condition develops or continues over time | Requires long-term medicines, monitoring and lifestyle management |
Guideline-directed treatment | Medicines and other therapies are selected according to the type of heart failure | Can improve symptoms and reduce complications for suitable patients |
Daily monitoring | Patients track symptoms, weight and other changes | Helps identify fluid accumulation or worsening heart failure |
Cardiac rehabilitation | Supervised exercise, education and risk-factor management | May improve fitness, confidence and long-term self-management |
Advanced treatment | Devices, surgery, mechanical support or transplantation | May be considered when standard treatment is insufficient |
What Is Left Heart Failure?
Left heart failure is a clinical condition where the left ventricle becomes too weak, damaged, thickened, or stiff to efficiently pump oxygen-rich blood to the body or accept blood returning from the lungs.
Key takeaway: Left heart failure involves more than reduced pumping strength. The left ventricle may be weak, stiff or affected by a combination of contraction and relaxation problems.
Detailed Explanation
The left side of the heart contains two chambers:
- The left atrium
- The left ventricle
Oxygen-rich blood travels from the lungs into the left atrium. It then enters the left ventricle, which contracts and sends blood through the aorta to the rest of the body. The left ventricle normally generates enough pressure to supply the brain, kidneys, muscles and other organs. When the ventricle becomes weak, damaged, enlarged, thickened or stiff, it may no longer handle blood efficiently.
This may create two closely connected problems:
1. Reduced forward blood flow The heart may not pump enough blood to meet the body’s needs. This may contribute to:
- Fatigue and weakness
- Reduced stamina
- Cold hands or feet
- Dizziness
- Reduced kidney function
- Difficulty concentrating in some patients
- 2. Backward pressure toward the lungs When the left ventricle cannot accept or eject blood properly, pressure may increase in the left atrium and pulmonary veins. Fluid can then move into the lung tissues, causing:
- Shortness of breath
- Coughing or wheezing
- Difficulty breathing while lying flat
- Sudden nighttime breathlessness
- Pulmonary oedema in severe cases
The kidneys may also retain sodium and water when circulation is impaired, increasing blood volume and worsening congestion.
Is Left Heart Failure the Same as Congestive Heart Failure?
The terms are closely related but not identical; heart failure means the heart is not pumping adequately, while congestive heart failure refers to heart failure that is actively causing fluid accumulation in the lungs or other tissues.
Key takeaway: A patient can have left heart failure without obvious swelling during the early stages. As the condition progresses, fluid retention may become more noticeable.
Detailed Explanation
Heart failure means that the heart is not pumping or filling adequately. Left heart failure specifically refers to dysfunction affecting the left side of the heart.
Congestive heart failure generally refers to heart failure accompanied by fluid accumulation or congestion. Congestion may involve the lungs, legs, abdomen or other tissues. Long-standing left heart failure may also place additional pressure on the right side of the heart. This can eventually lead to right-sided or biventricular heart failure, with swelling in the legs, ankles or abdomen.
What Are the Main Types of Left Heart Failure?
Left heart failure is primarily classified by the left ventricular ejection fraction (EF)—the percentage of blood pumped out of the ventricle per heartbeat—categorized as reduced, mildly reduced, preserved, or improved.
Key takeaway: Ejection fraction helps describe how well the heart contracts, but it does not provide a complete picture of heart function. A person may have significant heart failure symptoms even when the ejection fraction is within the preserved range.
Detailed Explanation
Heart Failure With Reduced Ejection Fraction (HFrEF) It generally means that the left ventricular ejection fraction is 40% or lower. The heart muscle does not contract effectively, so less blood is ejected with each heartbeat. This has traditionally been called systolic heart failure. Possible causes include previous heart attack, coronary artery disease, dilated cardiomyopathy, myocarditis, long-standing high blood pressure, and severe heart-valve disease.
Heart Failure With Mildly Reduced Ejection Fraction (HFmrEF) The ejection fraction is generally between 41% and 49%. Patients in this group may have features that overlap with both reduced and preserved ejection-fraction heart failure.
Heart Failure With Preserved Ejection Fraction (HFpEF) The ejection fraction is generally 50% or higher, but the heart muscle may be thickened, stiff or unable to relax normally. The ventricle may therefore fill under abnormally high pressure even though the percentage of blood pumped out appears preserved. This has traditionally been called diastolic heart failure. HFpEF is often associated with high blood pressure, older age, obesity, diabetes, and atrial fibrillation.
Heart Failure With Improved Ejection Fraction Some patients who previously had a reduced ejection fraction improve after treatment. An improved ejection fraction does not necessarily mean that the underlying condition has been cured. Medicines may need to continue because heart function and symptoms can deteriorate again if treatment is stopped.
Acute Versus Chronic Left Heart Failure
Chronic left heart failure develops and persists slowly over time, requiring long-term management, whereas acute left heart failure occurs suddenly—often as a medical emergency—due to a rapid deterioration or a trigger like a heart attack.
Key takeaway: Acute pulmonary oedema is a medical emergency. It occurs when fluid rapidly accumulates in the lungs and severely interferes with breathing.
Detailed Explanation
Chronic left heart failure Symptoms may remain stable for a period and then gradually worsen. Patients usually require long-term treatment, symptom monitoring and regular follow-up.
Acute left heart failure Acute heart failure develops suddenly or represents a rapid worsening of chronic heart failure. It may be triggered by:
- A heart attack
- Severe uncontrolled blood pressure
- A dangerous arrhythmia
- Acute heart-valve dysfunction
- Infection or myocarditis
- Missed medicines or excess sodium/fluid intake
What Causes Left Heart Failure?
Left heart failure can be caused by any condition that damages or overworks the left ventricle, including coronary artery disease, chronic high blood pressure, cardiomyopathy, severe heart-valve disease, and abnormal heart rhythms.
Key takeaway: Identifying the underlying cause is important because some causes require specific, highly targeted treatments to resolve the heart failure.
Detailed Explanation
Left heart failure may develop from any condition that changes the structure of the left ventricle:
- Coronary artery disease: Reduced blood flow weakens the muscle. A heart attack may permanently damage part of the left ventricle, reducing its ability to contract.
- High blood pressure: Long-standing high blood pressure forces the left ventricle to pump against increased resistance, eventually causing it to become thick, stiff, and weak.
- Cardiomyopathy: Diseases of the heart muscle (dilated, hypertrophic, restrictive, or genetic).
- Heart-valve disease: Aortic stenosis, aortic regurgitation, mitral regurgitation, or mitral stenosis. A narrowed valve obstructs flow, while a leaking valve increases the volume of blood the ventricle must handle.
- Arrhythmias: Persistent rapid heart rhythms can weaken the muscle, while very slow rhythms reduce forward blood flow.
- Other causes: Congenital heart conditions, myocarditis (inflammation), diabetes and metabolic disease, thyroid disease, sleep apnoea, alcohol misuse, and toxic substances.
What Are the Symptoms of Left Heart Failure?
The most common symptoms of left heart failure include shortness of breath during activity, difficulty breathing while lying flat, waking up breathless at night, persistent coughing, extreme fatigue, and eventual fluid retention.
Key takeaway: The symptoms of left heart failure can resemble those of lung disease, anaemia, kidney problems and other conditions. A thorough medical evaluation is needed to identify the exact cause.
Detailed Explanation
Symptoms depend on how quickly the condition develops, how severely heart function is affected and whether fluid congestion is present.
- Shortness of breath during activity: May initially occur only during strenuous activity, but progresses to appearing while walking short distances, bathing, or resting.
- Difficulty breathing while lying flat (orthopnoea): Lying flat allows more fluid to return to the chest, worsening lung congestion. Patients may need extra pillows.
- Waking suddenly at night (paroxysmal nocturnal dyspnoea): Waking severely short of breath, needing to sit or stand to breathe.
- Persistent coughing or wheezing: Fluid in the lungs causes a dry cough that often worsens when lying down.
- Fatigue, weakness, and reduced exercise tolerance: Reduced cardiac output limits oxygen delivery to muscles.
- Rapid or irregular heartbeat: The heart beats faster in an attempt to maintain blood flow.
- Fluid retention and swelling: Causes ankle swelling, leg swelling, abdominal fullness, and rapid weight gain.
- Digestive and neurological symptoms: Nausea, poor appetite, confusion, and difficulty concentrating due to reduced circulation.
How Is Left Heart Failure Diagnosed?
Doctors diagnose left heart failure by combining a detailed medical history and physical examination with specific tests like an echocardiogram to measure ejection fraction, an ECG to check rhythm, and blood tests to evaluate organ function.
Key takeaway: An echocardiogram is one of the most important tests for identifying the exact type of heart failure and guiding your ongoing treatment plan.
Detailed Explanation
Evaluation generally combines:
- Medical history & Physical examination: Checking for signs of congestion in the lungs and neck veins, swelling, and abnormal heart sounds.
- Echocardiogram: Uses ultrasound to assess ejection fraction, ventricular size, heart-muscle thickness, and heart-valve function.
- Electrocardiogram (ECG): Records the heart’s electrical activity to identify arrhythmias or past heart attacks.
- Blood tests: Includes BNP or NT-proBNP (substances released when the heart is under pressure), kidney/liver function, thyroid function, and cholesterol.
- Chest X-ray: May show heart enlargement or fluid in the lungs.
- Coronary evaluation: Stress testing, CT coronary angiography, or invasive angiography to check for blocked arteries.
- Cardiac MRI: Provides highly detailed information about heart structure, scar tissue, and inflammation when the cause remains uncertain.
How Is Left Heart Failure Treated?
Left heart failure is treated through a personalized combination of prescription medicines to reduce fluid and protect the heart, rigorous lifestyle management, cardiac rehabilitation, and in some cases, implantable devices or surgery.
Key takeaway: No single treatment plan is appropriate for every patient. Management depends on the type of heart failure, ejection fraction, blood pressure, kidney function, and the underlying cause.
Detailed Explanation
Treatment has several connected goals:
- Relieve symptoms and reduce fluid congestion
- Improve daily functioning and quality of life
- Treat the underlying cause and slow disease progression
- Reduce hospital admissions and risk of dangerous rhythms
- Support longer-term survival where possible
Medicines for Left Heart Failure
Patients typically require a combination of medicines, including diuretics to remove fluid, and specialized drugs like ARNIs, Beta-blockers, MRAs, and SGLT2 inhibitors to actively protect the heart muscle and improve long-term outcomes.
Key takeaway: Heart-failure medicines should be selected and adjusted according to the patient’s clinical condition. A medicine that is beneficial for one type of heart failure may not be appropriate for another.
Detailed Explanation
- Diuretics: Help the kidneys remove excess sodium and water to reduce lung congestion and swelling. Doses must be carefully balanced.
- Angiotensin-receptor neprilysin inhibitors (ARNI): Recommended for suitable patients with reduced ejection fraction to influence blood-vessel tone and hormonal pathways.
- ACE inhibitors and ARBs: Relax blood vessels and reduce strain on the heart.
- Beta-blockers: Reduce heart rate and protect the heart from excessive stress-hormone stimulation, improving heart function over time.
- Mineralocorticoid-receptor antagonists (MRA): Block harmful hormonal effects and provide mild diuretic activity.
- SGLT2 inhibitors: Originally for diabetes, these are now crucial heart-failure treatments for appropriate patients across different ejection fractions.
- Other medicines: May include Ivabradine, Hydralazine, Digoxin, anticoagulants, or intravenous iron for documented deficiency.
Does Treatment Differ According to Ejection Fraction?
Yes, guideline-directed medical therapy for reduced ejection fraction (HFrEF) involves a specific four-pillar medication strategy, whereas treatment for preserved ejection fraction (HFpEF) focuses heavily on relieving congestion and managing underlying conditions.
Detailed Explanation
Treatment of reduced ejection fraction (HFrEF) For suitable patients, guideline-directed medical therapy commonly includes four principal medicine groups: an ARNI/ACE/ARB, a beta-blocker, an MRA, and an SGLT2 inhibitor, plus diuretics to control fluid.
Treatment of preserved ejection fraction (HFpEF) HFpEF treatment usually focuses on relieving congestion, controlling blood pressure, treating atrial fibrillation, managing diabetes, and addressing obesity. Because HFpEF has several possible underlying mechanisms, management must be heavily personalised.
Lifestyle and Daily Management
Managing left heart failure at home requires active daily participation, including monitoring daily weight to catch sudden fluid retention, managing sodium and fluid intake, and safely engaging in medically approved physical activity.
Key takeaway: A sudden weight increase of just a few pounds over a couple of days may indicate dangerous fluid accumulation that requires immediate medical adjustment.
Detailed Explanation
- Sodium guidance: Limit heavily salted foods to prevent fluid retention. Discuss salt substitutes with your doctor, as some contain potassium which can interact with medications.
- Fluid guidance: A fluid limit may be recommended for patients with significant congestion.
- Daily weight monitoring: Weigh yourself at the same time each morning. Weight gain and increasing ankle swelling indicate deteriorating heart failure.
- Physical activity: Appropriate regular activity improves cardiovascular fitness. Stop immediately if you experience chest pain or severe breathlessness.
- Smoking cessation & Alcohol: Smoking damages blood vessels. Alcohol can worsen cardiomyopathies.
- Nutrition & Sleep: Adopt a heart-healthy diet and address sleep issues like sleep apnoea.
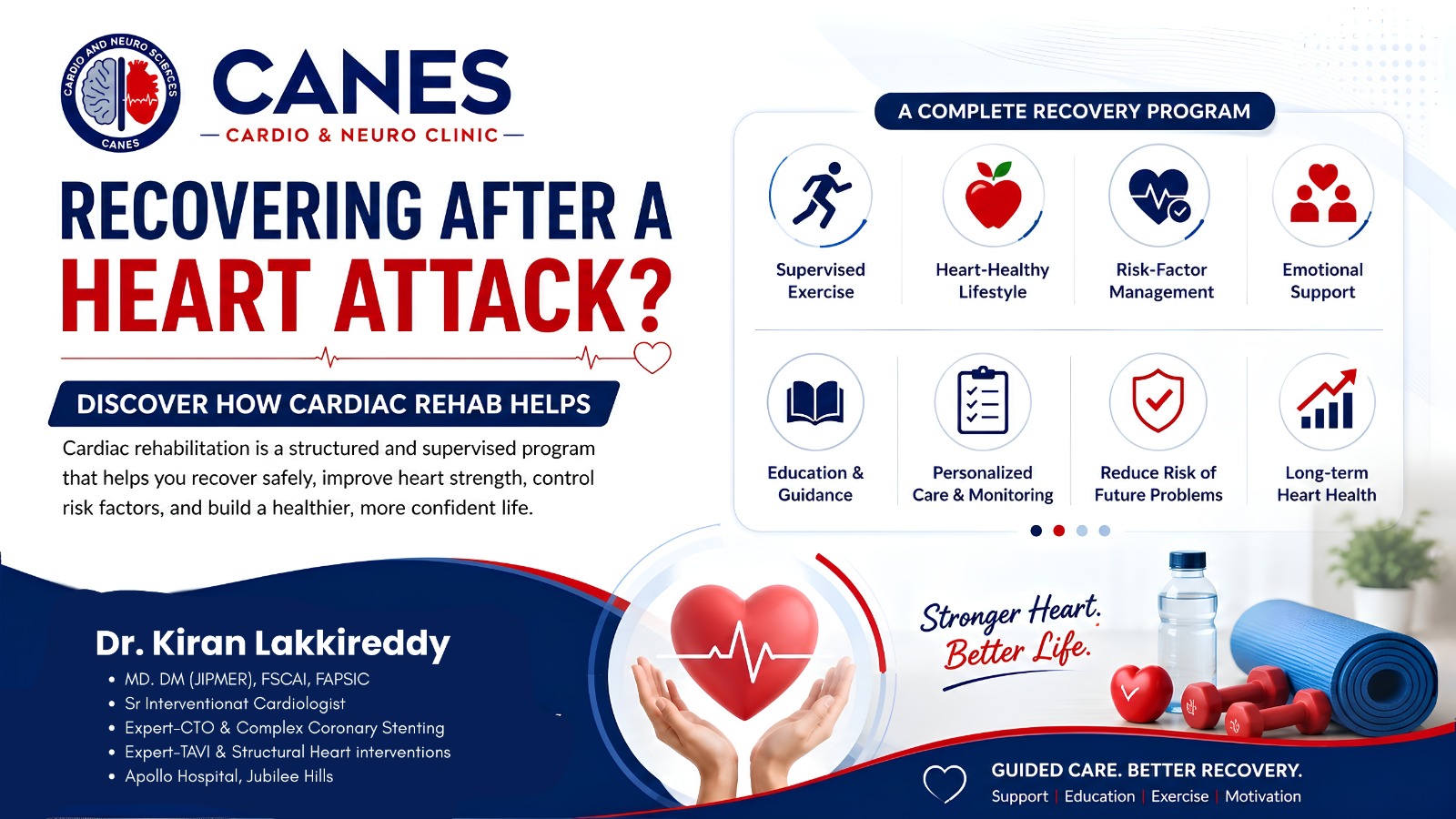
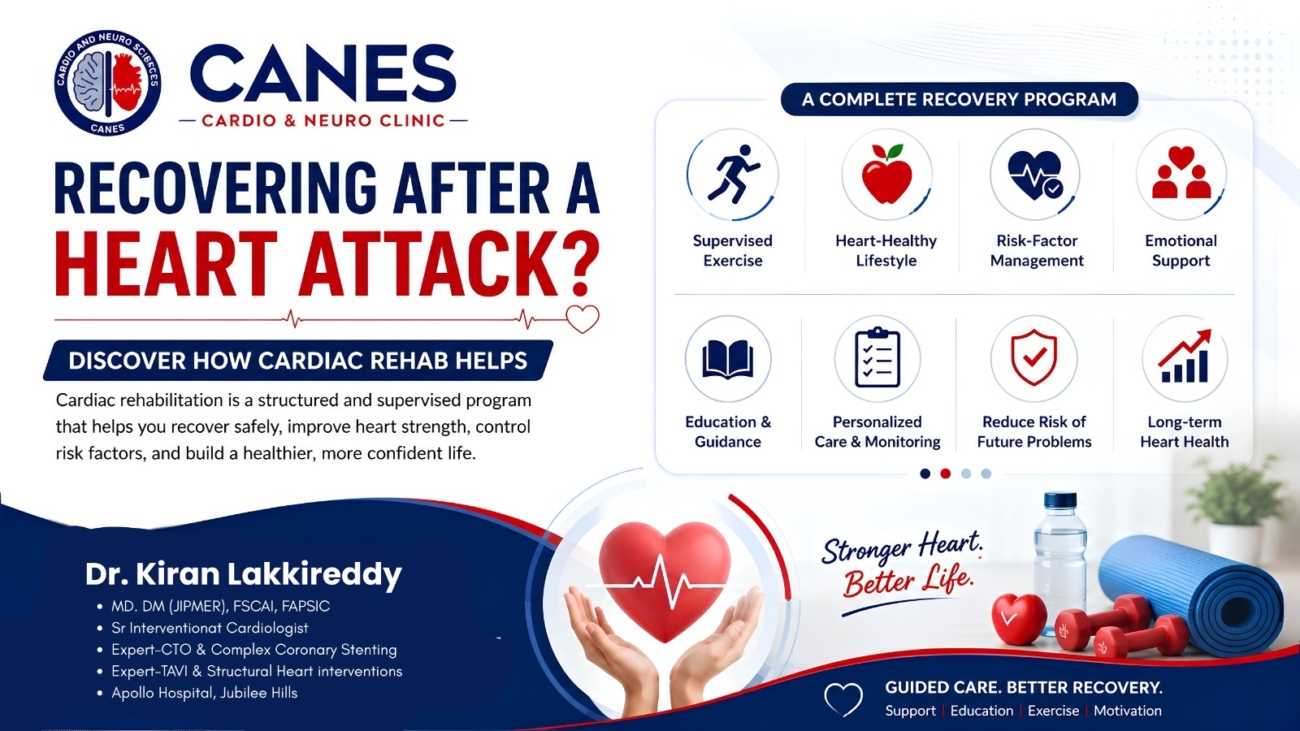
Cardiac Rehabilitation and Left Heart Failure
Cardiac rehabilitation is a highly recommended, medically supervised program that combines structured exercise, education on medicines and nutrition, and emotional support to help stable heart failure patients safely regain their physical confidence.
Key takeaway: Cardiac rehabilitation does not replace prescribed medicines or specialist care. It is a vital tool that supports physical recovery and long-term self-management.
Device Therapy, Procedures, and Surgery
When medicines alone are insufficient, doctors may utilize implantable devices like ICDs to prevent sudden cardiac arrest, specialized CRT pacemakers to coordinate heartbeats, or surgery to bypass blocked arteries and fix leaking valves.
Key takeaway: Not every patient with left heart failure needs an implanted device. Therapy depends entirely on your specific ejection fraction, electrical conduction patterns, and response to medical therapy.
Detailed Explanation
- Implantable cardioverter-defibrillator (ICD): Provides electrical treatment if it detects dangerous ventricular rhythms, reducing sudden cardiac arrest risk.
- Cardiac resynchronisation therapy (CRT): A specialised pacemaker that helps the ventricles contract in a more coordinated way for patients with a widened QRS complex.
- Coronary angioplasty (PCI) & Bypass surgery (CABG): Procedures to open or bypass blocked coronary arteries contributing to heart failure.
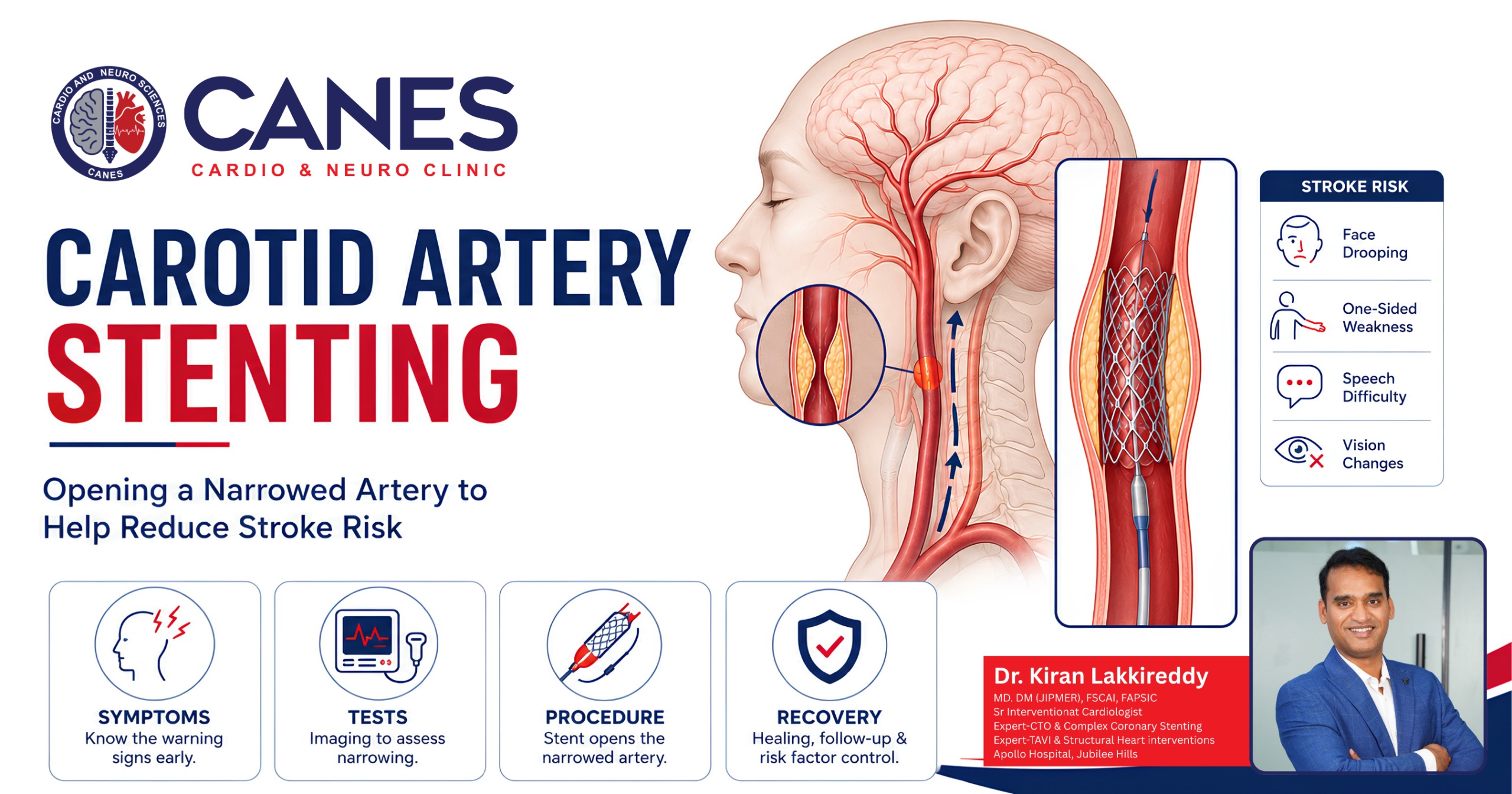
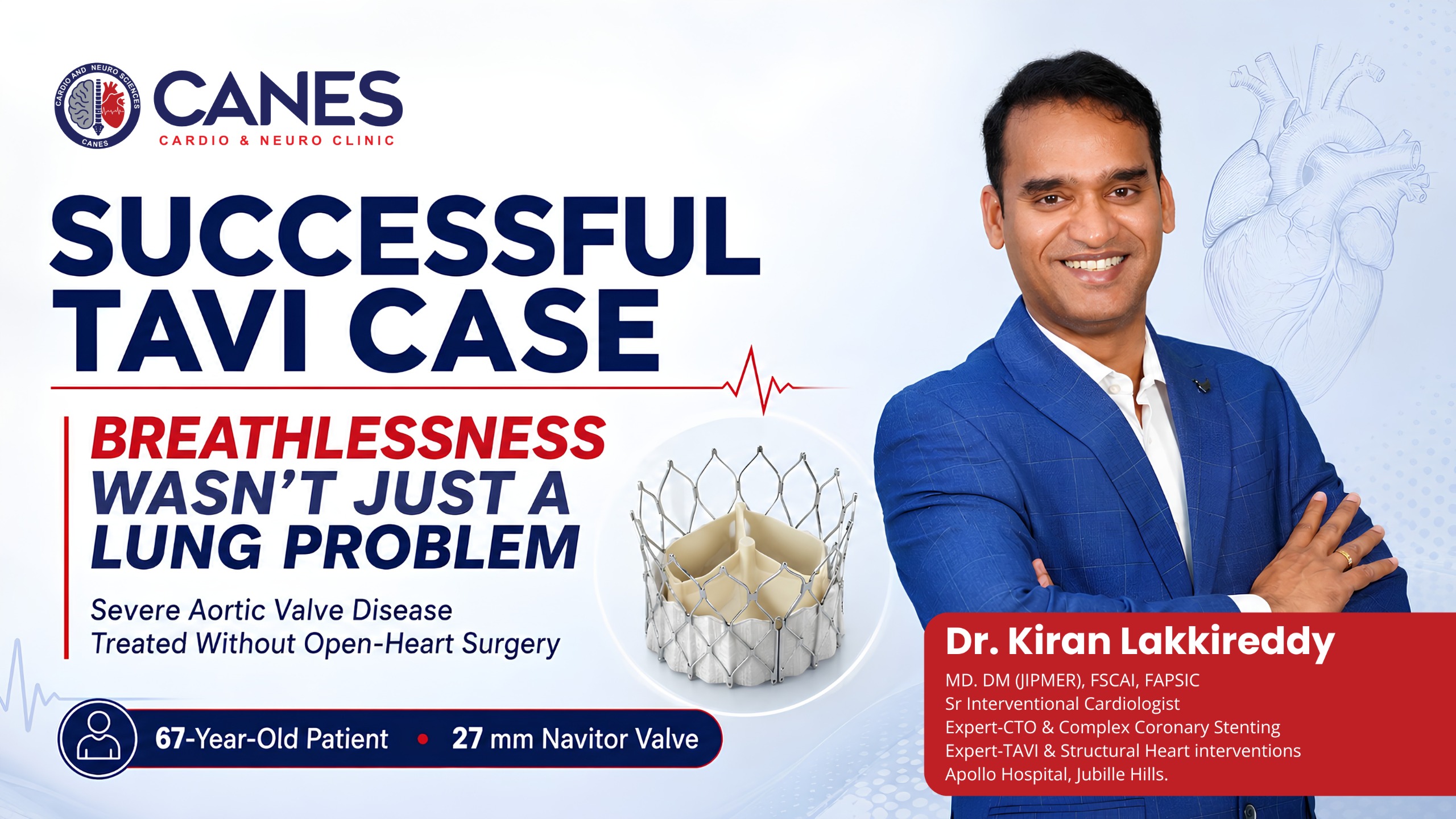
- Heart-valve repair or replacement: Surgical or transcatheter treatment for severe aortic or mitral valve disease.
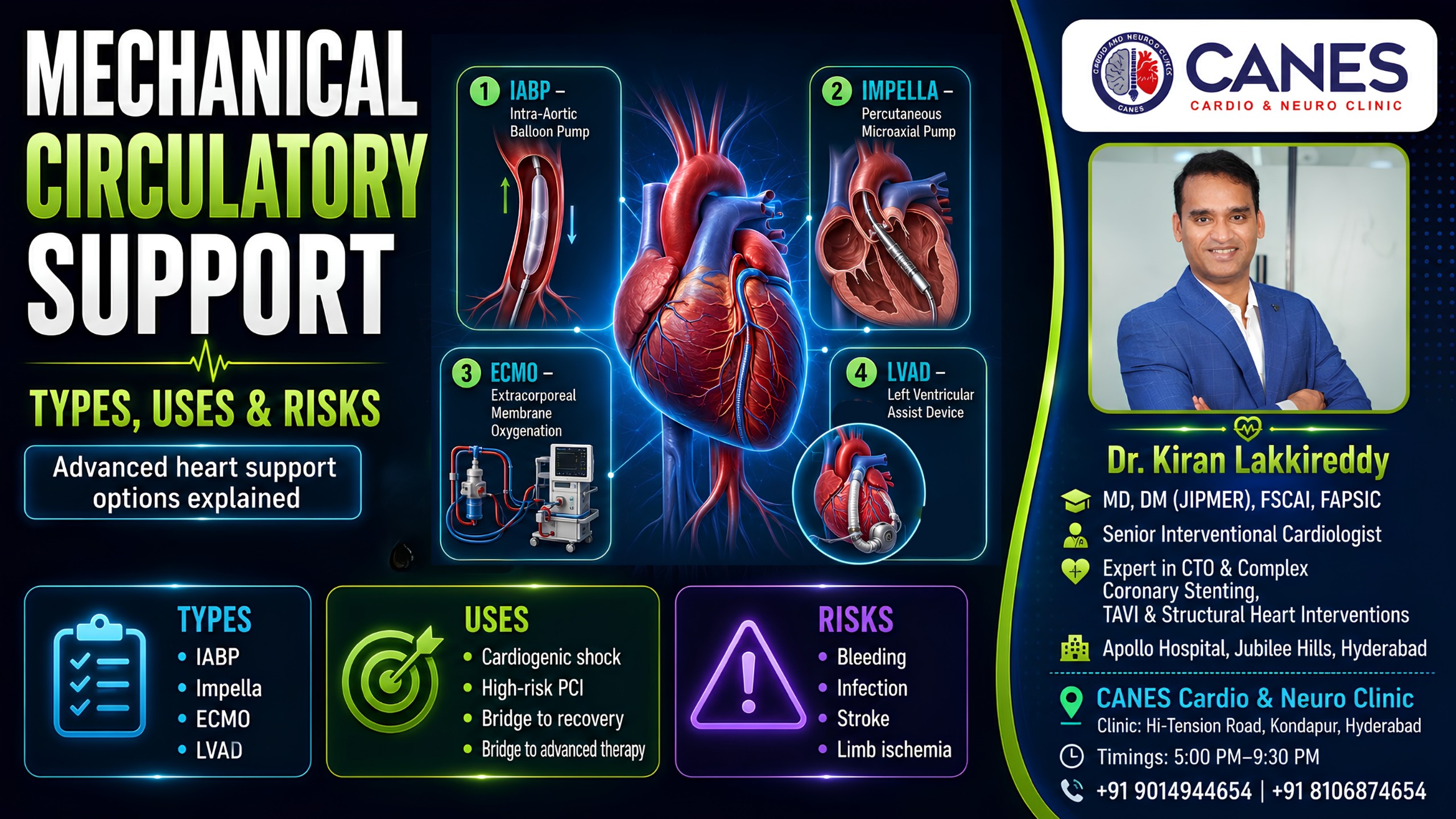
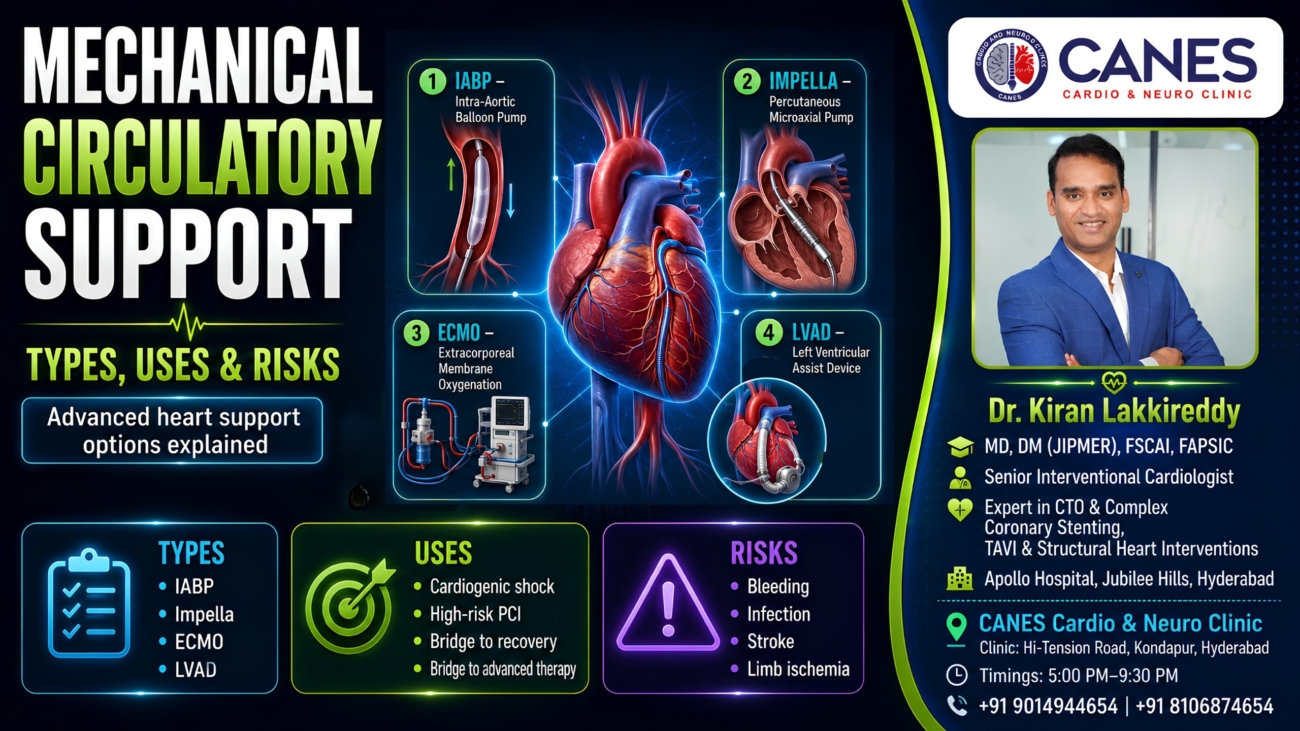
Advanced Left Heart Failure Therapies
For patients with advanced heart failure who continue to deteriorate despite all standard treatments, specialists may consider mechanical circulatory support (like an LVAD) or evaluation for a full heart transplantation.
Key takeaway: Timely referral to an advanced heart-failure team is recommended when symptoms remain severe, such as breathlessness at rest or progressive weight loss, allowing access to advanced therapies.
Can Left Heart Failure Be Cured?
While heart failure is generally a long-term, chronic condition, specific causes like rapid arrhythmias, blocked arteries, or treatable valve disease can improve substantially, and the heart’s pumping strength may recover with strict medical therapy.
Key takeaway: Even when heart function improves significantly on an echocardiogram, continued treatment and follow-up usually remain necessary to prevent the heart failure from returning.
What Are the Possible Complications?
If left untreated or poorly managed, left heart failure can rapidly lead to dangerous pulmonary oedema, kidney and liver dysfunction, severe arrhythmias, right heart failure, and sudden cardiac arrest.
Regular monitoring and early reporting of worsening symptoms (like sudden weight gain or new breathlessness) can help the healthcare team intervene before complications become life-threatening.
Emotional and Psychological Health
Living with chronic heart failure frequently causes significant anxiety, depression, and fear regarding physical limitations, making psychological support and counseling an essential component of comprehensive cardiovascular care.
Emotional support is part of comprehensive heart-failure care rather than a substitute for medical treatment. Seeking counseling or joining patient support groups can dramatically improve treatment participation and quality of life.
Myth vs. Fact: Left Heart Failure
Common Myth | Medical Fact |
|---|---|
Heart failure means the heart has stopped. | The heart is still beating, but it cannot pump or fill effectively enough to meet the body’s needs. |
Left heart failure always means a low ejection fraction. | Heart failure can occur with reduced, mildly reduced or preserved ejection fraction. |
A normal ejection fraction means the heart is completely normal. | A stiff ventricle may cause significant heart failure symptoms despite a preserved ejection fraction. |
Every patient has severe leg swelling. | Some patients mainly experience breathlessness and fatigue, particularly in earlier left-sided failure. |
Breathlessness is simply part of ageing. | New or worsening breathlessness requires assessment because it may indicate heart, lung or another medical problem. |
Feeling better means medicines can be stopped. | Symptoms can improve while the underlying condition remains. Medicines should not be stopped without medical advice. |
Exercise is unsafe for everyone with heart failure. | Appropriately selected, medically guided activity can be beneficial when the condition is stable. |
Actionable Checklist: What Should Patients Ask Their Cardiac-Care Team?
Use this checklist to ensure you fully understand your heart failure diagnosis and ongoing management plan:
- What is the likely cause of my left heart failure, and what is my specific ejection fraction?
- Do I have reduced, mildly reduced, or preserved ejection-fraction heart failure?
- Does my echocardiogram show a valve problem, or do I need testing for blocked arteries?
- Which of my medicines are intended to improve long-term outcomes, and which are primarily controlling fluid?
- How often should my kidney function and potassium be checked while taking these medications?
- Do I need a strict sodium or fluid limit, and what specific daily weight change should I report to the clinic immediately?
- What type of physical activity is safe for me, and am I a candidate for cardiac rehabilitation?
- Do I meet the criteria for an ICD, pacemaker, or CRT device assessment?
Cardiovascular Guidance at CANES Clinic
Left heart failure requires an individualised approach. The appropriate treatment plan depends on the underlying cause, ejection fraction, coronary artery disease, blood pressure, kidney function, and the patient’s recovery goals.
At CANES Cardio & Neuro Clinic, patients can receive structured cardiovascular evaluation and understandable guidance regarding heart conditions, risk-factor management and follow-up planning.
The clinic is guided by Dr. Kiran Lakkireddy, an experienced interventional cardiologist specialising in complex cardiology. The focus is on detailed assessment, patient education, shared decision-making and appropriate coordination with hospital-based heart-failure, electrophysiology, cardiac-surgery, and rehabilitation teams when necessary.
(Note: The clinic’s role should not be assumed to replace emergency hospital treatment, intensive care, advanced heart-failure services or a supervised cardiac rehabilitation programme.)
Location: 3rd Floor, Tapasavi Commercial Complex, Hi-Tension Road, Kondapur, Hyderabad
Contact: +91 9014944654
Appointment Booking: Visit CANES Clinic Official Portal
Specialist Profile: Dr. Kiran Lakkireddy Official Website
Key Points to Remember
- Left heart failure does not mean the heart has stopped: It means the left side cannot pump or fill effectively enough.
- Lung congestion is common: Increased pressure behind the left ventricle can cause breathlessness, coughing and difficulty lying flat.
- Ejection fraction helps classify heart failure: Left heart failure may occur with reduced, mildly reduced or preserved ejection fraction.
- A preserved ejection fraction does not exclude heart failure: The ventricle may be stiff and fill under high pressure.
- The underlying cause matters: Coronary disease, high blood pressure, cardiomyopathy, valve disease and arrhythmias require different treatment approaches.
- Medicines are individualised: Several medicine classes may be needed to control symptoms and protect the heart.
- Fluid monitoring is important: Sudden weight gain, swelling or increasing breathlessness may indicate worsening congestion.
- Follow-up remains necessary when symptoms improve: Heart function can deteriorate again if treatment or monitoring is discontinued.
- Severe symptoms are emergencies: Acute pulmonary oedema, heart attack and dangerous arrhythmias require immediate hospital care.
Frequently Asked Questions (FAQs)
It means that the left side of the heart cannot pump blood forward effectively or cannot relax and fill normally. This may reduce circulation to the body and increase pressure in the lungs.
No. Heart failure means impaired heart function, not that the heart has stopped. However, it is a serious condition that requires appropriate assessment and treatment.
No. A heart attack occurs when blood flow to part of the heart muscle is suddenly blocked. A heart attack can damage the left ventricle and lead to heart failure, but the conditions are not identical.
Yes. HFpEF can cause significant symptoms even when ejection fraction is 50% or higher. The problem may involve stiffness and abnormal filling rather than reduced contraction.
An ejection fraction of 40% or lower is generally classified as reduced. An EF from 41% to 49% is mildly reduced, while 50% or higher is considered preserved.
Yes. Ejection fraction may improve when the underlying cause is treated and appropriate medicines are followed consistently. Improvement varies between patients and does not automatically mean treatment can be stopped.
Pressure can build up in the blood vessels of the lungs when the left ventricle cannot handle blood effectively. Fluid may then enter the lung tissues, making breathing more difficult.
Lying flat can increase the return of blood and fluid toward the chest. A congested heart may struggle to handle this additional volume. Some patients therefore require extra pillows or need to sit upright.
Fluid that has accumulated in the legs during the day can move back toward the circulation while lying down. This may increase lung congestion and trigger sudden nighttime breathlessness.
No medicine should be stopped or changed without medical advice. Feeling better may mean that the treatment is working rather than that the underlying condition has disappeared.
Many stable patients can participate in appropriate physical activity. The programme should begin gradually and follow medical advice. Patients with acute or worsening symptoms should not begin strenuous exercise.
An ICD may be recommended for selected patients with significant risk of dangerous ventricular rhythms. The decision depends on ejection fraction, symptoms, cause, treatment duration and other clinical factors.
Expert Care
Hyderabad's leading Cardio & Neuro specialists.