● Lifestyle & Prevention
Risks of Heart Procedures: A Proven Guide to Patient Safety
Table of Contents
- Introduction
- Should I Be More Worried About the Procedure or the Heart Disease Itself?
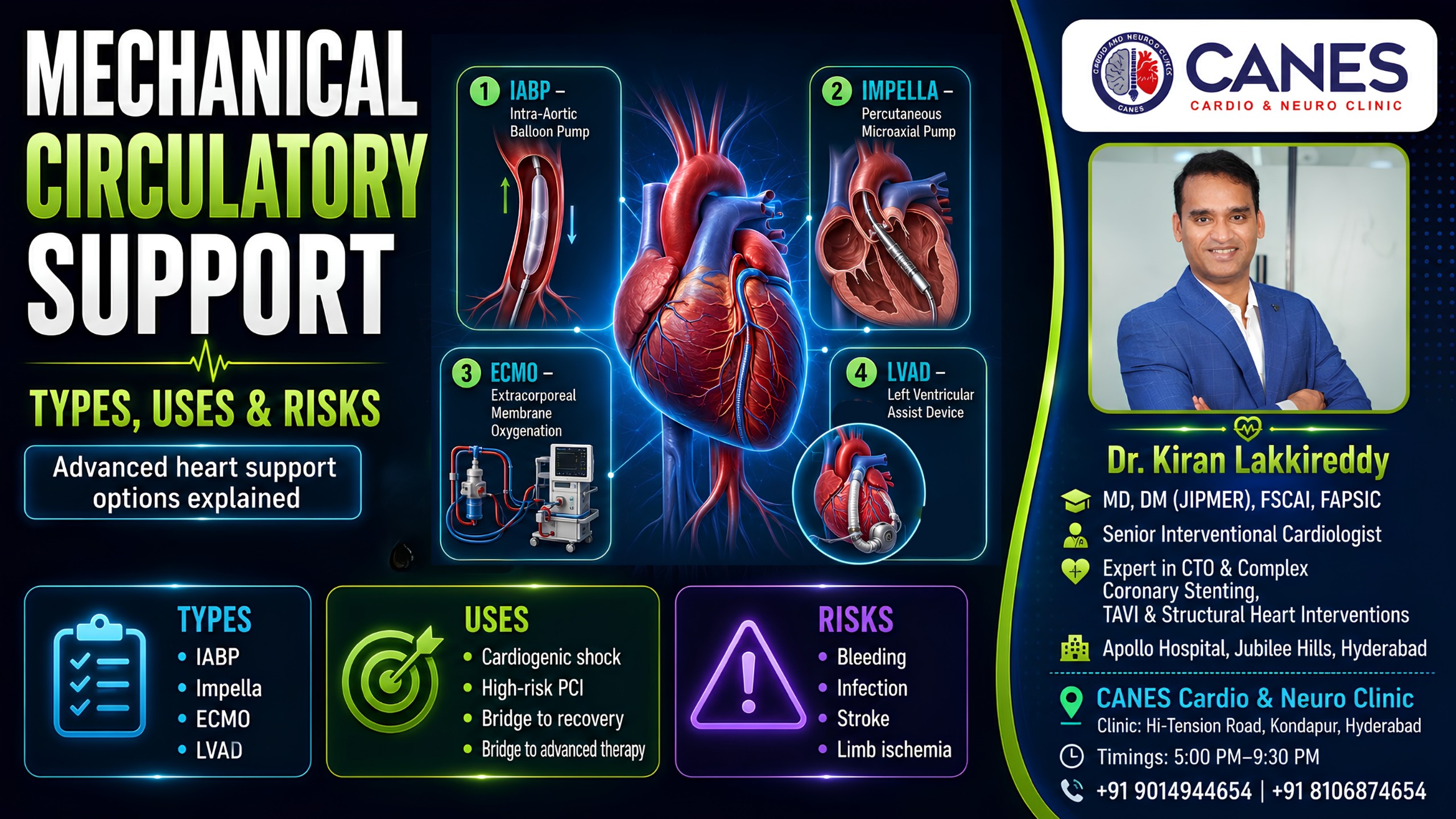
- What Are the Real Risks of Heart Procedures?
- What Is a Diagnostic Cardiac Catheterisation?
- What Are the Risks of Angioplasty and Stenting (PCI)?
- Why Are High-Risk PCI Procedures Different?
- What Are the Risks of a Permanent Pacemaker?
- How Do ICD and CRT Devices Compare to Pacemakers?
- What Is TAVI and What Are Its Safety Rates?
- What Is MitraClip Valve Repair?
- What Are the Risks of the Watchman Device (LAAO)?
- The Patient Safety Checklist: Preparing for Your Procedure
- What Questions Should You Ask Your Cardiologist?
- Expert Cardiac Care at CANES Clinic
- FAQs
Book a Consultation
Prevention is better than cure. Talk to our specialists today.
If your cardiologist has recommended an intervention, it is entirely natural to feel anxious about the risks of heart procedures. When you hear medical terms like “complications” or “surgery,” the fear of the unknown can quickly become overwhelming. However, when we look closely at the actual medical data, the numbers are incredibly reassuring. Most modern cardiac interventions are minimally invasive, highly routine, and designed with your long-term safety as the absolute top priority.
By understanding exactly what these procedures involve and looking at the real chances of complications based on published medical research, you can replace fear with confident, informed decision-making. At CANES Cardio & Neuro Clinic, guided by Dr. Kiran Lakkireddy, we believe in absolute transparency. This comprehensive guide will clearly explain the anatomical purpose of each treatment, the published statistics, and the specific safety protocols your care team uses to protect you.
Quick Answer
While all medical interventions carry some level of risk, the risks of heart procedures are generally very low for planned, routine cases. On average, diagnostic tests and standard stenting have a major complication rate of less than 1%. Modern cardiology relies heavily on minimally invasive catheter techniques, which significantly reduce the chances of severe bleeding, infection, and prolonged recovery compared to traditional open-heart surgery.
Should I Be More Worried About the Procedure or the Heart Disease Itself?
For most patients, untreated heart disease carries a significantly greater risk of permanent disability or death than the actual procedure designed to treat it.
Key Takeaway: The risks of heart procedures are closely managed and monitored by a medical team, whereas the progression of an untreated blocked artery or a failing valve is highly unpredictable and often fatal.
It is completely normal to focus on the immediate anxiety of entering a hospital. However, it is vital to weigh that short-term anxiety against the long-term reality of your condition. If a cardiologist recommends a stent or a valve repair, it is because your heart is currently in a dangerous, unstable state.
Declining a necessary intervention means leaving a severe blockage or electrical fault untreated. This dramatically increases your daily risk of suffering a sudden, massive heart attack, developing irreversible heart failure, or experiencing a fatal cardiac arrest. Medical interventions are recommended only when the benefit of fixing the heart overwhelmingly outweighs the statistical risk of the procedure.
What Are the Real Risks of Heart Procedures?
The real risks of heart procedures depend entirely on your specific heart condition, your age, and whether the procedure is planned or an emergency. However, on average, the risk of a major complication for a routine intervention is exceptionally low, often sitting below 1%.
Key Takeaway: The complication numbers you see online are population averages; your personal risk may be much lower, which is why your care team takes specific steps to keep those numbers as low as possible for you.
When reading through this guide, remember that numbers can be reassuring once you see them in proper medical context. A 1% risk means that out of 100 people, 99 experience absolutely no severe issues. Furthermore, your cardiology team spends extensive time planning your specific procedure to mitigate any personal health challenges, such as existing kidney issues or a history of bleeding.
Visual Scale: Procedure Risk Levels
To help put things into perspective quickly, here is how cardiologists generally classify the risk levels of common interventions.
Procedure | Average Risk Level |
|---|---|
Diagnostic Angiogram | Very Low |
Routine PCI (Stenting) | Low |
Permanent Pacemaker | Low |
TAVI (Valve Replacement) | Moderate |
High-Risk PCI | Higher |
What Is a Diagnostic Cardiac Catheterisation?
A diagnostic cardiac catheterisation (angiogram) is a test where a thin tube is guided through your wrist or groin, and contrast dye is injected to make your arteries show up clearly on an X-ray. It lets your doctor see exactly where any blockages are.
Key Takeaway: This is the most basic heart procedure and is often the very first step before anything else is done, carrying a mortality risk of just 0.05–0.1% in planned cases.
This is a very safe procedure. The risk of mortality is around 0.05–0.1% for planned (elective) cases, rising to about 1% only in emergency situations. A heart attack or stroke during the test is similarly rare at 0.05–0.1%.
The more common issues are minor. Bruising or a small lump at the access site occurs in 1–3% of people having the test through the groin, and less than 0.5% through the wrist (which is why many doctors prefer using the wrist). Some people have a mild allergic reaction to the contrast dye—about 1–3%—though severe reactions are extremely rare. The dye can also occasionally affect your kidneys temporarily, more so if you already have kidney problems.
What Are the Risks of Angioplasty and Stenting (PCI)?
Percutaneous Coronary Intervention (PCI) is a procedure where a small balloon is inflated to open a blocked artery, and a stent (a tiny mesh tube) is left in place to keep the artery open. It restores blood flow without open-heart surgery.
Key Takeaway: For planned PCI in stable patients, the risk of death is exceptionally low, around 0.1–0.5%. It remains the safest and most effective way to clear a blocked artery.
If the catheterisation shows a blocked artery, PCI is often done at the same time. If you are having PCI during an active heart attack, the risk is naturally higher—around 3–7%—because you are already unwell when the procedure starts. A small number of patients, about 1–3%, experience a minor heart attack signal during the procedure itself, often without any physical symptoms.
The stent can occasionally clot off in the days afterward (stent thrombosis), affecting around 0.5–1.5% of patients. This is exactly why it is so important to keep taking your blood-thinning medication as prescribed; stopping early is the main cause of this complication. Over the longer term, the artery can re-narrow (restenosis) in 5–10% of people, even with modern drug-coated stents.
Why Are High-Risk PCI Procedures Different?
High-risk PCI is performed on patients with severe underlying problems, such as a very weak heart muscle, heavily calcified arteries, or cardiogenic shock. These cases require extra support equipment and are reviewed by a full team of specialists.
Key Takeaway: The elevated risks of heart procedures in this category reflect how sick the patient’s heart already was, rather than the procedure itself causing the danger.
Because the underlying heart condition is much more serious, the risks are understandably higher. In-hospital death ranges from 3–10% in stable high-risk patients. However, it can be as high as 20–50% if someone arrives already in cardiogenic shock.
Roughly 2–5% of patients have a significant heart attack during the procedure, and about 3–8% may develop or worsen shock. Mechanical heart support devices, when used, carry their own risks (around 5–10%), such as reduced blood flow to the leg where the device is inserted.
What Are the Risks of a Permanent Pacemaker?
A permanent pacemaker is a small device placed under the skin near your collarbone, with wires running into your heart to keep your heart rate steady when it is beating too slowly.
Key Takeaway: This is a well-established, low-risk procedure with a death rate under 0.1%, offering a highly reliable solution for slow heart rhythms.
The most common complications are a small blood collection at the implant site (2–5%) and minor infection of the wound (1–2%). Both are usually manageable without major treatment.
More serious infection of the device or leads happens in about 0.5–1% of cases and would need the device to be removed and replaced. Occasionally, a wire can shift out of position (1–3%) and need repositioning. A collapsed lung from the vein puncture during insertion happens in 0.5–2% of cases. The device itself typically lasts 10–15 years before the battery needs replacing.
How Do ICD and CRT Devices Compare to Pacemakers?
An ICD can deliver a shock to correct a dangerous rapid heart rhythm, while a CRT adds an extra wire to help both sides of your heart beat in better coordination for heart failure.
Key Takeaway: These devices are more complex than standard pacemakers, meaning the procedural risks are slightly higher (death around 0.1–0.5%).
The trickiest part of CRT implantation is placing the third wire on the left side of the heart. This anatomical challenge fails in about 5–10% of attempts, and even when successful, the wire can shift position afterward in up to 10% of cases.
One of the more emotionally difficult complications is an inappropriate shock—where the device fires when it did not need to. This happens in roughly 5–10% of patients per year, though settings are usually adjusted afterward to reduce this. About 20–30% of CRT patients do not notice the symptom improvement they were hoping for; this is called non-response and is a limitation of the therapy rather than a complication.
At a Glance: Comparing the Risks of Heart Procedures
Procedure Type | Primary Purpose | Average Mortality Risk | Most Common Minor Issue |
|---|---|---|---|
Diagnostic Angiogram | Locate blockages | 0.05–0.1% (Planned) | Bruising at access site (1-3%) |
Routine PCI (Stenting) | Open blocked artery | 0.1–0.5% (Stable) | Artery re-narrowing over time |
Permanent Pacemaker | Fix slow heartbeats | < 0.1% | Small blood collection (2-5%) |
TAVI Valve Replacement | Replace aortic valve | 1–2% (Low risk) | Needing a new pacemaker (10-25%) |
What Is TAVI and What Are Its Safety Rates?
TAVI replaces a worn-out aortic valve through a catheter, usually via the groin, without open-heart surgery. It is typically offered to people whose surgical risk is too high for traditional operations, though it is increasingly used for lower-risk patients too.
Key Takeaway: TAVI provides a life-saving alternative to open surgery with death rates within 30 days ranging from 1–2% in lower-risk patients to 2–5% in higher-risk patients.
Stroke occurs in 2–5% of patients within the first month. One of the more common after-effects is needing a permanent pacemaker afterward because the new expanding valve can disrupt your heart’s electrical pathways; this happens in 10–25% of cases depending on the device used.
Some leakage around the new valve (paravalvular leak) is seen in 3–10% of patients, and major complications at the artery access site occur in 3–7%. Serious complications like the valve frame tearing the aortic annulus are rare, under 1%, but are treated as emergencies when they occur.
What Is MitraClip Valve Repair?
MitraClip treats a leaking mitral valve by clipping the two leaflets together so they close more effectively, done through a catheter from the groin under general anaesthesia.
Key Takeaway: Mortality within 30 days is around 1–3% for degenerative valve disease and 3–7% for heart failure patients, offering symptom relief without open-chest trauma.
The clip occasionally only grips one of the two leaflets properly (single leaflet attachment) in about 3–8% of cases, which can mean the leak is not reduced as much as hoped. In 10–15% of patients, some degree of leakage remains after the procedure. Serious complications from the catheter crossing into the left side of the heart, such as a fluid buildup around the heart, occur in 0.5–2% of cases.
What Are the Risks of the Watchman Device (LAAO)?
The Watchman device seals off a small pouch in the heart where blood clots tend to form in people with atrial fibrillation, offering a permanent alternative to taking long-term blood thinners.
Key Takeaway: This is one of the lower-risk structural procedures available, with an average mortality rate well under 1%.
Fluid around the heart requiring drainage occurs in 1–3% of cases. A small clot can form on the surface of the device itself in 3–7% of patients, which is exactly why you will usually stay on some blood-thinning medication for a period after the procedure, even though the goal is to eventually stop it. Stroke around the time of the procedure occurs in just 1–2% of cases.
Myth vs. Fact: Common Myths About Heart Procedures
Understanding the true risks of heart procedures means separating internet myths from proven medical facts.
Common Myth | Medical Fact |
|---|---|
All heart procedures are highly dangerous. | Most planned, routine procedures have major complication rates well below 1%. |
Stents cure heart disease permanently. | Stents fix blockages, but lifestyle changes and medication are required to prevent new ones. |
Pacemakers stop the heart from failing. | Pacemakers regulate the electrical rhythm, not the physical pumping strength of the heart muscle. |
Open-heart surgery is the only way to fix valves. | Advanced structural techniques like TAVI can now replace valves through a tiny catheter. |
The Patient Safety Checklist: Preparing for Your Procedure
Minimizing the risks of heart procedures requires teamwork between you and your doctor. Use this actionable checklist to prepare safely:
Review Medications: Provide your doctor with a complete list of all prescriptions, especially blood thinners and diabetes medications.
Check Kidney Function: Ensure you have recent blood work done so your doctor knows exactly how well your kidneys will handle the contrast dye.
Report Allergies: Clearly state any allergies you have to iodine, shellfish, or previously used anesthetics.
Plan Your Discharge: Arrange for a trusted family member or friend to drive you home and monitor you for the first 24 hours.
What Questions Should You Ask Your Cardiologist?
Every number above is a population average. Your own personal risk depends entirely on your specific heart condition, your age, your other health conditions, and how the procedure is performed. If you are due to have any of these procedures, it is worth asking your doctor:
- What is my specific, personal risk percentage based on my current health profile?
- What would realistically happen to my heart if I chose not to have this procedure?
- What specific steps does the surgical team take to reduce these risks for someone in my situation?
A good conversation with your cardiologist before the day of the procedure is one of the best ways to walk in feeling informed rather than just nervous.
Expert Cardiac Care at CANES Clinic
Navigating a cardiac diagnosis requires a medical team that combines technical precision with open, empathetic communication. At CANES Cardio & Neuro Clinic, we prioritize thorough patient education and evidence-based procedural care. We understand that discussing surgical risks can cause anxiety, and we are dedicated to providing clear, authoritative answers.
Guided by Dr. Kiran Lakkireddy, an experienced interventional cardiologist specializing in complex structural heart procedures, our facility ensures that every diagnostic angle is fully explored. Whether you require a routine angiogram, complex high-risk stenting, or advanced pacemaker management in Hyderabad, our team utilizes the latest protocols to keep your personal risk as low as absolutely possible.
Location: 3rd Floor, Tapasavi Commercial Complex, Hi-Tension Rd, Kondapur, Hyderabad
Contact: +91 9014944654
Appointment Booking: Visit CANES Clinic Official Portal
Learn More About Our Specialist: Dr. Kiran Lakkireddy Official Website
(Disclaimer: This article is for general educational purposes and is not a substitute for personalised medical advice. Always discuss your individual risks and options with your treating cardiologist.)
Key Points to Remember
Context Matters: Published complication rates are averages; your specific risk profile depends heavily on your age and the severity of your heart disease.
Routine vs. Emergency: Planned, elective procedures like standard angiograms carry extremely low complication risks, while emergency interventions inherently carry higher risks.
Medication is Crucial: Taking your prescribed antiplatelet medication after a stent is placed is the most important step you can take to prevent dangerous blood clots.
Structural Alternatives: Advanced techniques like TAVI and MitraClip offer patients life-saving valve repairs through a simple catheter, completely avoiding the severe trauma of open-heart surgery.
Frequently Asked Questions (FAQs)
Is it normal to feel chest pain during a stent procedure?
Yes, it is very common to feel a brief sensation of chest pressure or mild pain exactly at the moment the cardiologist inflates the balloon inside your artery. This pressure typically resolves as soon as the balloon is deflated.
How long does it take to recover from a cardiac catheterisation?
If the procedure was performed through your wrist, recovery is very fast; you can typically walk immediately and go home the same day. If accessed through the groin, you will need to lie completely flat for a few hours.
Can a pacemaker be affected by household appliances like microwaves?
Modern pacemakers have excellent internal shielding. Standard household appliances, including microwaves and televisions, are completely safe to use without interfering with your device.
Why do I need blood thinners after getting a stent if the blockage is fixed?
A new metal stent is seen as a “foreign object” by your immune system. Blood thinners prevent blood platelets from sticking to the bare metal and forming a dangerous clot before your body naturally heals over it.
What is the difference between a pacemaker and an ICD?
A pacemaker is designed only to speed up a heart that is beating too slowly. An ICD does this as well, but it also has the ability to deliver a strong internal shock to stop a chaotic, dangerously fast heart rhythm.
Are the risks of TAVI lower than traditional open-heart valve surgery?
For many patients, especially the elderly or those with multiple health conditions, TAVI is significantly safer than open-heart surgery because it avoids the need for a heart-lung bypass machine and large chest incisions.
Expert Care
Hyderabad's leading Cardio & Neuro specialists.