● Lifestyle & Prevention
Why Chronic Total Occlusions (CTOs) Need to Be Opened: An Evidence-Based Perspective
Table of Contents
- Introduction
- What Exactly Are Chronic Total Occlusions?
- Why Should Chronic Total Occlusions Be Opened?
- What Happens If Chronic Total Occlusions Are Not Opened?
- Which CTOs Should Be Opened?
- Who May Not Benefit From CTO PCI?
- What Investigations Are Required Before Opening a CTO?
- Actionable Checklist: What Should You Do Next?
- Expert CTO Interventions at CANES Clinic
- FAQs
Book a Consultation
Prevention is better than cure. Talk to our specialists today.
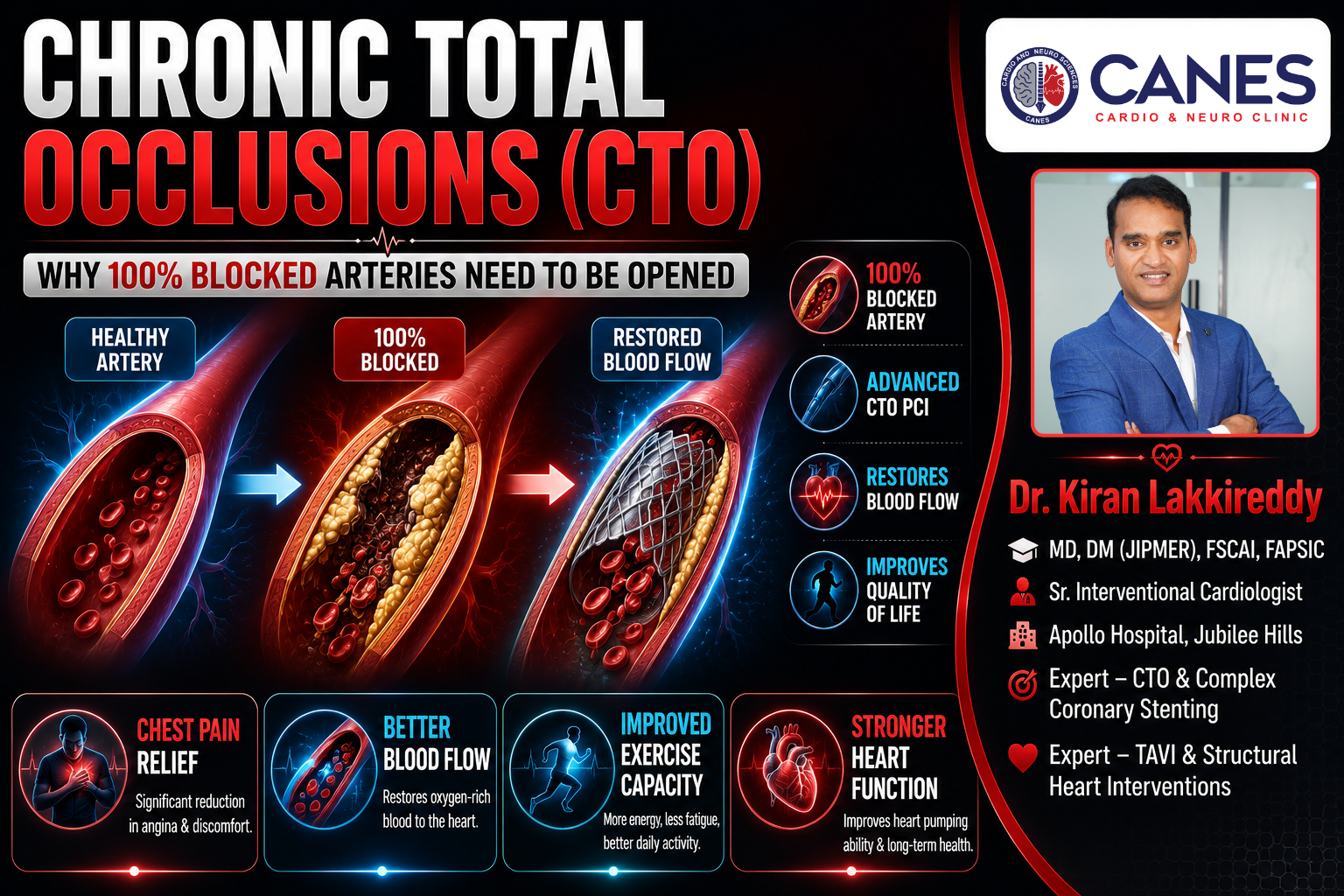
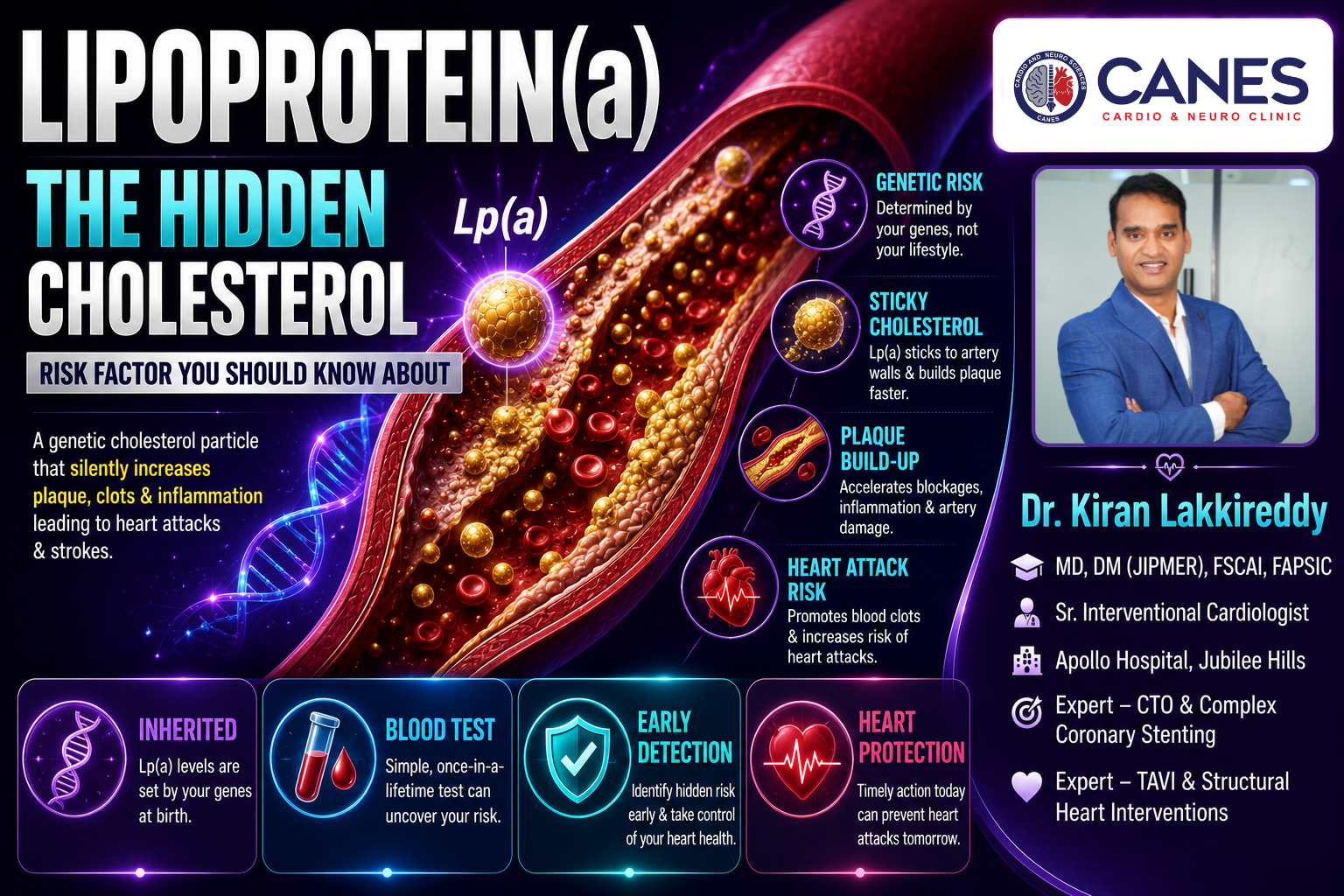
Receiving a diagnosis of a completely blocked heart artery can sound terrifying, but modern cardiology has evolved significantly to treat complex conditions. A Chronic Total Occlusion (CTO) is a complete blockage of a coronary artery that has been present for at least three months. Unlike sudden blockages that cause acute heart attacks, Chronic Total Occlusions develop gradually. Because they grow slowly, your body attempts to adapt by forming tiny, fragile detour blood vessels called collaterals to bypass the blockage.
However, these collateral vessels are rarely enough. When you walk, exercise, or experience stress, these small detour pathways cannot deliver enough oxygen-rich blood to your heart muscle. As a result, patients frequently experience severe chest pain, extreme fatigue, and a progressive deterioration of their overall heart function.
At CANES Cardio & Neuro Clinic in Hyderabad, guided by Dr. Kiran Lakkireddy, we specialize in advanced interventional cardiology. Today, a highly specialized procedure known as CTO Percutaneous Coronary Intervention (CTO PCI) can safely and successfully open these chronic blockages. In this comprehensive, evidence-based guide, we will explore exactly why opening Chronic Total Occlusions is necessary, who benefits the most, and who might safely avoid the procedure.
Quick Answer
Chronic Total Occlusions are 100% blocked arteries that have been closed for months or years, causing the heart to starve for oxygen. Opening a CTO using a specialized stenting procedure (CTO PCI) restores essential blood flow to the heart muscle. This minimally invasive procedure significantly relieves chest pain, improves your ability to exercise, protects your long-term heart function from deteriorating, and dramatically improves your overall quality of life.
What Exactly Are Chronic Total Occlusions?
Chronic Total Occlusions are 100% complete blockages in a main coronary artery that have existed for more than 90 days, typically composed of heavily calcified, hardened cholesterol plaque.
Key Takeaway: A CTO is a long-standing, hardened roadblock in your artery that forces your heart to rely on inefficient, temporary detour vessels for blood supply.
Quick Answer
To understand Chronic Total Occlusions, imagine a major highway that has been completely blocked by a landslide for months. Over time, drivers start using small, unpaved backroads to get around the blockage. In your heart, these backroads are called “collateral vessels.”
While these collaterals are an amazing natural defense mechanism that keeps the heart muscle alive, they are fundamentally inadequate. They are too small to carry the high volume of blood your heart needs when it works hard. As a result, the heart muscle supplied by the blocked artery remains alive but “hibernating” it is constantly starving for oxygen, which causes symptoms like severe breathlessness and chest pain (angina) during physical exertion.
Why Should Chronic Total Occlusions Be Opened?
The primary goal of a CTO PCI procedure is to eliminate the roadblock and restore normal, high-volume blood flow to the deprived heart muscle, which immediately improves symptoms and long-term cardiac function.
Key Takeaway: Opening a CTO wakes up hibernating heart muscle, drastically improving your daily energy levels and reducing your dependence on temporary collateral vessels.
Quick Answer
Advances in interventional cardiology mean that experienced centers now achieve success rates exceeding 85–95% for CTO PCI. Revascularization (opening the artery) provides several evidence-based clinical benefits:
- Relief of Angina and Symptoms: Patients with a CTO frequently experience severe chest pain, reduced exercise capacity, and profound fatigue. Multiple randomized clinical trials have proven that successful CTO revascularization significantly reduces angina frequency and improves daily physical functioning.
- Improvement in Left Ventricular Function: The heart muscle below the blockage is often viable but functionally paralyzed (hibernating myocardium). Restoring normal blood flow wakes this tissue up, improving the heart’s overall pumping strength (Left Ventricular Ejection Fraction) and stopping the heart from dangerously enlarging.
- Reduction in Ischemic Burden: Opening the main artery physically reduces the total area of the heart that is starving for oxygen (ischemia). Patients with a large ischemic burden derive the absolute greatest survival benefit from this procedure.
- Improved Quality of Life: The most immediate and profound benefit reported by patients is a massive upgrade in their quality of life. Patients can return to physical activity, experience less breathlessness, and significantly reduce their daily anti-anginal medications.
What Happens If Chronic Total Occlusions Are Not Opened?
Leaving significant Chronic Total Occlusions untreated often leads to a progressive worsening of daily chest pain, dangerous weakening of the heart muscle, and a significantly higher risk of developing congestive heart failure.
Key Takeaway: While collaterals keep the muscle alive temporarily, relying on them long-term causes the heart muscle to scar, weaken, and eventually fail.
Quick Answer
Ignoring a significant blockage that is actively starving a large portion of the heart carries severe long-term consequences:
Progressive Heart Failure: Long-standing oxygen deprivation causes the heart muscle to develop irreversible scar tissue (fibrosis). The heart compensates by remodeling and stretching out, which eventually leads to congestive heart failure.
Ventricular Arrhythmias: Scarred, ischemic heart tissue becomes highly unstable. This acts as an arrhythmogenic substrate, meaning it can trigger dangerous, chaotic heart rhythms (like ventricular tachycardia) that can lead to sudden cardiac death.
Greater Dependence on Collaterals: Collateral circulation often looks impressive on an angiogram but rarely provides normal perfusion. Over time, if these tiny collateral vessels fail or become diseased themselves, the dependent heart muscle will inevitably die.
Which CTOs Should Be Opened?
International cardiology guidelines recommend CTO PCI in carefully selected patients, particularly those with persistent symptoms, demonstrable ischemia, and viable myocardium.
Key Takeaway: Careful patient selection is the most critical step; the procedure is reserved for patients where restoring blood flow will clearly and meaningfully improve their heart function or daily life.
Detailed Explanation
Not every blocked artery is a candidate for this advanced procedure. A specialized cardiologist will evaluate you against strict clinical criteria to ensure the intervention is medically beneficial:
Symptomatic Patients: You experience exercise limitation, dyspnea (breathlessness), or persistent angina despite taking optimal medical therapy.
Large Ischemic Burden: Medical imaging shows that a significant portion of your total heart muscle (typically >10%) is currently starving for oxygen due to the blockage.
Viable Myocardium: Testing confirms that the heart muscle below the blockage is merely “hibernating” and not permanently scarred. If the tissue is already completely dead, placing a stent will not bring it back.
Who May Not Benefit From CTO PCI?
Not every 100% blocked artery requires an intervention. Patients without symptoms, those with extensive irreversible scar tissue, or individuals whose overall health makes the procedural risks outweigh the benefits may be safely managed with medications and careful follow-up.
Key Takeaway: An expert cardiologist exercises balanced clinical judgment; they will only perform CTO PCI if the physiological benefits of restoring blood flow are proven to outweigh the risks.
Detailed Explanation
While CTO PCI is a life-changing procedure for highly symptomatic patients, patient selection is central to current evidence-based practice. Interventional cardiologists carefully evaluate who might not benefit from the procedure to avoid unnecessary risks.
If a patient is completely asymptomatic meaning they have absolutely zero chest pain and excellent physical stamina despite the blockage the risks of a complex intervention may outweigh the benefits. Furthermore, if advanced imaging (like a Cardiac MRI) reveals that the heart muscle supplied by the blocked artery has already turned into 100% dense, irreversible scar tissue, opening the artery will unfortunately not restore any heart function. In these specific scenarios, relying on optimal medical therapy and careful observation is often the safest and most effective long-term strategy.
Common Myths About Chronic Total Occlusions
Myth | Medical Fact |
|---|---|
A 100% blocked artery means the heart muscle is already dead. | Many CTOs have collateral blood flow that keeps the muscle alive but “hibernating” for years. |
CTOs can only be fixed with open-heart bypass surgery. | Modern CTO PCI allows experts to open chronic blockages minimally invasively using advanced catheters. |
If I don’t feel pain, the blockage isn’t causing damage. | Silent ischemia can slowly destroy your heart muscle and lead to heart failure without causing chest pain. |
What Investigations Are Required Before Opening a CTO?
Before attempting to open Chronic Total Occlusions, a cardiologist will order advanced imaging such as Cardiac MRI, PET scans, or CT Coronary Angiography to definitively prove that the heart muscle is viable and to create a precise 3D map of the hardened blockage.
Key Takeaway: Procedural success relies heavily on meticulous pre-planning using advanced imaging to understand the length, hardness, and exact location of the occlusion.
Detailed Explanation
Because a CTO is a hard, chronic roadblock, the procedural planning is extensive. You will undergo several critical tests to ensure the procedure is safe and appropriate:
- Diagnostic Coronary Angiography: This is the baseline X-ray test to visually confirm the anatomy of the Chronic Total Occlusions, assess the quality of the collateral vessels, and calculate clinical scoring systems (like the J-CTO Score) to predict procedural complexity.
- Stress Cardiac MRI: Considered the gold standard for viability assessment. An MRI precisely quantifies how much of the heart muscle is healthy, how much is ischemic, and the exact percentage of permanent transmural scar tissue.
- Nuclear Perfusion Imaging (PET/SPECT): Highly useful for quantifying the exact ischemic burden and predicting how much functional benefit you will get from revascularization.
- Coronary CT Angiography (CTCA): This advanced scan provides a detailed 3D roadmap of the artery. It allows the operator to measure the exact length of the CTO, identify heavy calcium deposits, and navigate vessel tortuosity before they even begin the physical procedure.
Actionable Checklist: What Should You Do Next?
If you or a loved one has been diagnosed with a 100% blocked artery, taking proactive steps before your consultation ensures you get the absolute best care plan possible.
Gather Old Records: Bring the physical CD or USB drive of your previous angiograms. Looking at paper reports is not enough; the CTO specialist must see the actual moving video of your arteries.
List Your Symptoms: Write down exactly what physical activities cause your chest to feel tight or make you feel breathless (e.g., “I can only walk 2 blocks before stopping”).
Request Viability Testing: Ask your cardiologist if a Cardiac MRI or PET scan is appropriate to prove your heart muscle is still alive and “hibernating.”
Seek a Second Opinion: Ensure your chosen interventional cardiologist has specific, high-volume training in advanced CTO PCI techniques, as this drastically improves success rates.
Expert CTO Interventions at CANES Clinic
Conquering Chronic Total Occlusions requires a medical facility equipped with cutting-edge technology and a clinical team possessing extraordinary technical skill. At CANES Cardio & Neuro Clinic, we pride ourselves on tackling the cardiovascular cases that other centers consider “too complex.” We believe that no patient should be forced to live a restricted, painful life if their heart muscle is still viable and waiting to be rescued.
Guided by Dr. Kiran Lakkireddy, an exceptionally experienced interventional cardiologist, our clinic utilizes state-of-the-art imaging and the most advanced micro-catheter techniques available globally. We approach every CTO systematically, ensuring that patient safety and long-term functional recovery are our highest priorities. By accurately assessing ischemic burden and myocardial viability, we deliver highly personalized, life-changing results.
Location: 3rd Floor, Tapasavi Commercial Complex, Hi-Tension Rd, Kondapur, Hyderabad
Contact: +91 9014944654
Appointment Booking: Visit the CANES Clinic Official Portal
Specialist Profile: Dr. Kiran Lakkireddy Official Website
Key Points to Remember
- The Slow Blockage: Chronic Total Occlusions are 100% blocked arteries that have been closed for over three months, causing the heart to survive on tiny, inefficient backup collateral vessels.
- Hibernating Muscle: The lack of blood flow causes the heart muscle to “sleep” and lose pumping strength, which leads to chronic fatigue, severe angina, and breathlessness.
- Advanced Revascularization: Opening the blockage through CTO PCI wakes up the hibernating muscle, vastly improving heart function and giving you your active life back.
- Patient Selection is Key: The procedure is highly recommended for patients who have persistent physical symptoms and a proven large area of viable, living heart muscle.
- High Success Rates: In the hands of a dedicated CTO specialist using modern micro-tools, the success rate for safely opening these complex blockages exceeds 85–95%.
Frequently Asked Questions (FAQs)
Is a CTO procedure safe for elderly patients?
Yes, CTO PCI is frequently and safely performed on elderly patients. Because it is minimally invasive and performed through the wrist or groin, it avoids the heavy trauma of open-heart surgery, making it highly suitable for older adults with symptomatic limitations.
How long does a typical CTO PCI procedure take?
Because drilling through old, calcified plaque requires extreme precision and patience, a CTO procedure typically takes longer than a standard stent placement, often lasting anywhere from 2 to 4 hours depending on the complexity.
Can Chronic Total Occlusions be managed with medication alone?
While medications can help manage the symptoms of angina and control blood pressure, they absolutely cannot dissolve a hard, calcified CTO. If your physical symptoms restrict your daily life, medication alone is failing to manage the disease adequately.
Will I have to stay in the hospital for a long time after the procedure?
No. Most patients recover remarkably quickly. If the procedure is uncomplicated, patients are typically monitored overnight for safety and are discharged to go home the very next day.
What is the "retrograde approach" in CTO surgery?
The retrograde approach is an advanced technique where the cardiologist threads a microscopic wire through your tiny collateral backup vessels to attack the back end of the hard blockage, which is often much softer and easier to penetrate than the front end.
Will I still need to take blood thinners after my CTO is opened?
Yes. Just like any standard stenting procedure, you will be required to take dual antiplatelet therapy (blood thinners like aspirin and Clopidogrel or Ticagrelor) for a specific period to ensure a dangerous blood clot does not form inside the new metal stent.
Expert Care
Hyderabad's leading Cardio & Neuro specialists.