● Lifestyle & Prevention
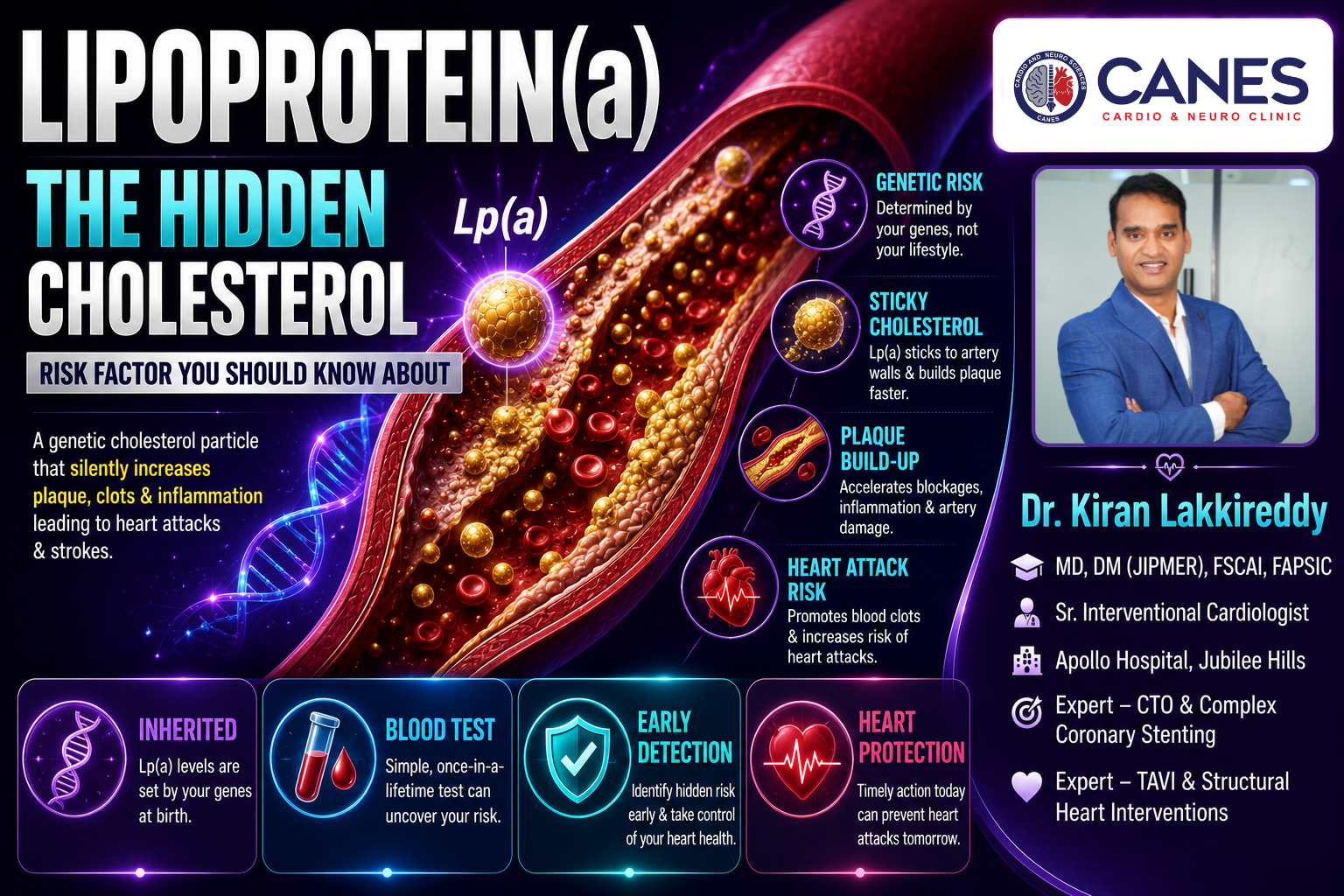
Lipoprotein(a): The Hidden Cholesterol Risk Factor You Should Know About
Table of Contents
- Introduction
- What Is Lipoprotein(a)?
- Why Do Some Healthy People Get Heart Attacks?
- How Does Lipoprotein(a) Cause Heart Attacks?
- When Should You Speak to a Cardiologist About Lipoprotein(a)?
- What Is Considered a High Lipoprotein(a) Level?
- Should I Be More Concerned About My Lp(a) Levels or My LDL Cholesterol?
- Can Lifestyle Changes Lower Lipoprotein(a)?
- Can Medications Reduce Lipoprotein(a)?
- Myth vs. Fact: Understanding Lipoprotein(a)
- Advanced Preventive Cardiology at CANES Clinic
- FAQs
Book a Consultation
Prevention is better than cure. Talk to our specialists today.
Heart attacks are traditionally linked to well-known lifestyle factors like high blood pressure, smoking, diabetes, and a poor diet. However, there is another critical, largely invisible factor that many patients and even some doctors overlook: Lipoprotein(a). Commonly referred to as Lp(a), this unique type of cholesterol particle is determined almost entirely by your genetics, not by what you eat.
It is incredibly frustrating for patients who lead a perfectly healthy lifestyle, exercise daily, and maintain normal weight to suddenly suffer a cardiovascular event. Often, an overlooked contributor to these sudden emergencies is elevated Lipoprotein(a). Understanding this hidden risk factor is essential for identifying vulnerable individuals much earlier in life and preventing serious, unexpected cardiovascular events.
At CANES Cardio & Neuro Clinic, a specialized center for preventive cardiovascular care in Hyderabad, we believe in providing our patients with the most comprehensive metabolic screening available. Guided by Dr. Kiran Lakkireddy, an experienced interventional cardiologist, our goal is to help you uncover your true cardiovascular risk. In this clear, evidence-based guide, we will explain exactly what Lp(a) is, why it threatens otherwise healthy people, and the modern medical protocols used to manage it.
Quick Answer
Lipoprotein(a) is a highly dangerous, genetically inherited type of cholesterol that significantly accelerates plaque buildup, blood clotting, and inflammation in the arteries. Unlike standard “bad” cholesterol (LDL), Lp(a) levels cannot be lowered by traditional diet or exercise. Identifying high levels through a simple, once-in-a-lifetime blood test allows cardiologists to aggressively manage your overall heart health and prevent early heart attacks and strokes.
What Is Lipoprotein(a)?
Lipoprotein(a), pronounced “Lipoprotein little a,” is a specialized, cholesterol-carrying particle in the blood that consists of an LDL (bad cholesterol) molecule attached to an extra, highly sticky protein called apolipoprotein(a). This unique structure makes it much more dangerous to the arteries than standard cholesterol.
Key Takeaway: The extra sticky protein attached to Lp(a) allows it to easily bind to blood vessel walls, rapidly accelerating the formation of dangerous blockages.
Quick Answer
To understand why this specific particle is so concerning, you have to look at its biological structure. Lipoprotein(a) is essentially a standard LDL cholesterol molecule that has been genetically modified. It carries an extra protein loop called apolipoprotein(a). This added protein completely changes how the molecule behaves inside your cardiovascular system.
Standard LDL cholesterol causes harm over many decades. However, the extra protein on Lp(a) makes the particle highly adhesive. It acts like molecular velcro, readily sticking to the inner lining of your arteries and rapidly dumping its cholesterol payload. Furthermore, because the size and amount of Lp(a) in your blood are dictated entirely by the genes you inherited from your parents, your levels are determined at birth and remain relatively stable throughout your entire life.
Cholesterol Particles At a Glance
Particle Type | Primary Function | Clinical Impact |
|---|---|---|
LDL | Transports fat to cells. | Forms slow-growing plaques; heavily influenced by diet. |
HDL | Transports fat back to the liver. | Protects arteries; acts as a microscopic cleaning system. |
Lipoprotein(a) | Genetically altered LDL. | Highly sticky; accelerates rapid plaque growth and blood clots. |
Why Do Some Healthy People Get Heart Attacks?
Many healthy individuals suffer unexpected heart attacks because they have inherited high levels of Lipoprotein(a), which silently damages their arteries over many years despite normal blood pressure, a healthy weight, and regular exercise.
Key Takeaway: If you have a strong family history of premature heart disease but live a healthy lifestyle, high Lp(a) is frequently the undetected genetic culprit.
Quick Answer
One of the most confusing scenarios in cardiology is the patient who does everything right they do not smoke, they run marathons, and they eat a strict, plant-based diet yet they still require a stent at age 45. Traditional cholesterol panels (which only measure total cholesterol, standard LDL, HDL, and triglycerides) will often show perfectly normal numbers for these patients.
Because a standard lipid panel does not automatically check for Lipoprotein(a), this hidden risk factor remains invisible. The high levels of Lp(a) silently and aggressively drive inflammation and plaque formation inside the coronary arteries for decades without causing a single physical symptom. It is only when the plaque eventually ruptures and causes a heart attack that the underlying genetic risk is finally investigated.
How Does Lipoprotein(a) Cause Heart Attacks?
Lipoprotein(a) directly causes heart attacks through a dangerous three-step mechanism: it rapidly builds cholesterol plaques, creates severe inflammation inside the artery wall, and chemically promotes the formation of blood clots.
Key Takeaway: Lp(a) is a triple threat to your cardiovascular system, simultaneously blocking the artery, irritating the tissue, and encouraging sudden blood clots.
Quick Answer
Lp(a) contributes to severe, early-onset heart disease through three highly specific biological mechanisms:
- Accelerated Plaque Formation: Because of its sticky nature, Lp(a) easily penetrates the delicate inner lining of the blood vessels. Once inside, it deposits heavy amounts of cholesterol, narrowing the blood vessel much faster than standard LDL.
- Vascular Inflammation: The unique structure of Lp(a) carries oxidized, inflammatory molecules directly into the artery wall. This chronic irritation makes the existing plaques highly unstable and prone to sudden rupturing.
- Blood Clot Promotion: The extra protein on Lp(a)—apolipoprotein(a)—structurally mimics a natural protein in your body that breaks down blood clots. Because it looks similar, it blocks the body’s natural clot-dissolving process. Therefore, if a plaque tears, a blood clot forms rapidly and is much harder for the body to dissolve, leading directly to a complete blockage and a heart attack.
When Should You Speak to a Cardiologist About Lipoprotein(a)?
You should seek an evaluation from a cardiologist if you have a family history of early heart attacks, suffer from unexplained premature strokes, have relatives with familial hypercholesterolemia, or struggle with stubbornly high LDL cholesterol despite taking medication.
Key Takeaway: Because your Lp(a) levels are determined by your DNA, global cardiology guidelines now suggest every adult should undergo this specific blood test at least once in their life.
The Diagnostic Checklist
While universal testing is ideal, an experienced cardiologist will strongly recommend immediate Lp(a) testing if you meet any of the following clinical criteria:
- Family History: You have a close relative who suffered a heart attack or required a stent at an early age (men under 55, women under 65).
- Unexplained Events: You have suffered a heart attack or a premature stroke despite having “perfect” standard cholesterol numbers and a healthy lifestyle.
- Medication Resistance: You take statins or other cholesterol medications, but your standard LDL cholesterol remains stubbornly high.
- Genetic Conditions: You or a family member have been diagnosed with familial hypercholesterolemia (an inherited condition causing very high total cholesterol).
- Valve Disease: You have been diagnosed with early-onset aortic valve stenosis (a stiffening and narrowing of the heart valve).
What Is Considered a High Lipoprotein(a) Level?
While laboratory measurement units can vary, a Lipoprotein(a) level below 30 mg/dL is generally considered low risk, while levels above 50 mg/dL indicate a significantly high risk for cardiovascular disease.
Key Takeaway: The higher your Lp(a) level rises above the 50 mg/dL threshold, the more aggressively your cardiologist must manage your overall cardiovascular health.
Lp(a) Risk Categories
Lp(a) Blood Level | Clinical Risk Category | Medical Action Required |
|---|---|---|
Less than 30 mg/dL | Low Risk | Standard, routine cardiovascular monitoring. |
30 – 50 mg/dL | Intermediate Risk | Monitor closely; aggressively optimize lifestyle factors. |
Above 50 mg/dL | High Risk | Strict intervention required; aggressive control of all other risk factors. |
(Note: Some laboratories measure Lp(a) in nanomoles per liter (nmol/L). In this unit, levels above 125 nmol/L are generally considered high risk.)
Should I Be More Concerned About My Lp(a) Levels or My LDL Cholesterol?
You should view both markers as a combined, cumulative risk; while you cannot easily change your genetic Lp(a) levels, keeping your standard LDL cholesterol as low as possible helps offset the overall danger to your arteries.
Key Takeaway: Do not panic over a high Lp(a) result. Instead, use it as powerful motivation to keep all your other, controllable cardiovascular risks absolutely perfect.
Detailed Explanation
It is easy for patients to feel defeated upon discovering they have a high, genetic Lipoprotein(a) level. However, cardiovascular disease relies on total risk accumulation. Think of your blood vessels as a boat taking on water. If your genetics (Lp(a)) represent a leak you cannot easily plug, you must relentlessly bail out the other water (LDL cholesterol, high blood pressure, blood sugar) to keep the boat safely afloat.
If your Lp(a) is elevated, your cardiologist will likely become highly aggressive in lowering your standard LDL cholesterol to targets well below normal guidelines (often below 55 mg/dL). By minimizing the standard plaque-building material in your blood, you drastically reduce the overall workload and stress on your arteries, keeping you safe despite the genetic risk.
Can Lifestyle Changes Lower Lipoprotein(a)?
Unfortunately, unlike standard cholesterol, your Lipoprotein(a) levels are not significantly reduced by adopting a healthy diet, losing weight, or exercising regularly. Because the levels are hardwired into your genetics, lifestyle modifications cannot alter the production of this specific particle.
Key Takeaway: While a healthy diet will not lower your Lp(a) number, eating well and exercising are absolutely critical to prevent additional inflammation and damage to your cardiovascular system.
Detailed Explanation
Patients are often frustrated to learn that a strict Mediterranean diet or running daily will not lower their Lp(a) blood test results. However, this absolutely does not mean lifestyle is irrelevant.
Because you carry a higher baseline risk, maintaining pristine cardiovascular health through lifestyle is non-negotiable. Regular aerobic exercise keeps the blood vessels flexible. A diet rich in plant-based antioxidants actively lowers the systemic inflammation that Lp(a) tries to cause. Strictly avoiding tobacco prevents additional chemical damage to the arterial walls, and maintaining a healthy weight prevents diabetes, which acts as a massive accelerant for plaque rupture.
Can Medications Reduce Lipoprotein(a)?
Traditional cholesterol medications like statins do not effectively lower Lipoprotein(a); however, advanced injectable therapies (PCSK9 inhibitors) and highly promising new genetic medications currently in clinical trials have shown success in reducing Lp(a) levels.
Key Takeaway: While standard pills cannot eliminate Lp(a), the medical landscape is rapidly evolving, and highly targeted therapies are actively entering clinical use.
Detailed Explanation
Managing high Lipoprotein(a) requires specialized knowledge, as standard protocols do not apply. An experienced cardiologist will guide you through the current and emerging pharmacological options:
Shared Decision-Making: Management depends entirely on your overall cardiovascular risk, family history, existing heart disease, and other laboratory findings, rather than the Lp(a) level alone. Treatment plans are highly individualized.
Statins: While highly effective at lowering standard LDL and reducing overall heart attack risk, statins have virtually zero impact on lowering Lp(a) levels. However, they are still heavily prescribed to high-Lp(a) patients to offset total cardiovascular risk.
PCSK9 Inhibitors: These are advanced, injectable cholesterol-lowering medications (such as Repatha or Praluent). While primarily designed to aggressively lower LDL, clinical data shows they also reliably reduce Lp(a) by approximately 20% to 30%.
Emerging RNA Therapies: The future of Lp(a) treatment is incredibly bright. Several new drugs specifically target the messenger RNA in the liver to halt the production of the apolipoprotein(a) protein. Early clinical trials show these drugs can dramatically reduce Lp(a) levels by up to 80%.
Myth vs. Fact: Understanding Lipoprotein(a)
Separating internet myths from proven medical facts is essential when dealing with a genetic risk factor like Lipoprotein(a).
Common Myth | Medical Fact |
|---|---|
A standard cholesterol test checks for Lp(a). | No, a basic lipid panel only checks total cholesterol, LDL, HDL, and triglycerides. Lp(a) requires a specific, separate blood test. |
I can lower my Lp(a) by eating less saturated fat. | Lp(a) is almost entirely genetic. Diet significantly lowers standard LDL but has virtually zero effect on Lp(a). |
High Lp(a) only causes heart attacks. | It is also a primary driver of strokes, peripheral artery disease, and early narrowing of the aortic heart valve (aortic stenosis). |
If I have high Lp(a), a heart attack is inevitable. | High Lp(a) is a risk factor, not a guarantee. Aggressive management of blood pressure and LDL drastically lowers your risk. |
Advanced Preventive Cardiology at CANES Clinic
Discovering a hidden genetic risk factor requires a medical team that combines diagnostic precision with calm, structured, and compassionate support. At CANES Cardio & Neuro Clinic, we prioritize thorough patient education and evidence-based care paths above all else. We understand that finding out you have a genetic cardiovascular risk can cause anxiety, and we are dedicated to providing clear, authoritative answers and proactive solutions.
Guided by Dr. Kiran Lakkireddy, an experienced specialist in complex cardiology, our facility offers advanced cardiovascular screenings that go far beyond standard cholesterol checks. By utilizing comprehensive lipid testing, including Lipoprotein(a) assays, we uncover your true baseline risk. If you have a family history of early heart disease or have suffered an unexplained cardiac event, scheduling a specialized evaluation is a vital step toward protecting your long-term health.
Location: 3rd Floor, Tapasavi Commercial Complex, Hi-Tension Rd, Kondapur, Hyderabad
Contact: +91 9014944654
Appointment Booking: Visit the CANES Clinic Official Portal
Specialist Profile: Dr. Kiran Lakkireddy Official Website
Key Points to Remember
The Hidden Threat: Lipoprotein(a) is a genetically inherited, highly sticky cholesterol particle that aggressively accelerates plaque buildup and blood clotting.
Invisible on Standard Tests: You can have perfect standard cholesterol numbers but still carry a high risk of a heart attack due to elevated Lp(a).
One-Time Testing: Because Lp(a) levels are determined by your DNA, global guidelines suggest every adult should undergo this specific blood test at least once in their life.
Offsetting the Risk: While diet cannot lower Lp(a), aggressively controlling your blood pressure, standard LDL cholesterol, and blood sugar is the best way to keep your heart safe.
What Should You Do Next?
- If you are concerned about your cardiovascular health or have a family history of heart disease, taking proactive steps today can protect your future.
- Ask your doctor if you have ever had a specific Lipoprotein(a) blood test included in your lipid panels.
- Review your family history to identify if any close relatives suffered from early heart attacks, strokes, or required stents at a young age.
- Keep your standard LDL cholesterol as low as possible under medical supervision if your Lp(a) is elevated.
- Continue healthy lifestyle habits (exercise, good diet, no smoking) to reduce overall arterial inflammation, even though they do not directly lower Lp(a) levels.
Frequently Asked Questions (FAQs)
Can I lower my Lipoprotein(a) naturally by taking Niacin or Fish Oil supplements?
No. Clinical trials have shown that standard over-the-counter supplements like fish oil (Omega-3s) do not reduce Lp(a) levels. While very high, prescription doses of Niacin can cause mild reductions, the side effects are often severe, and it does not actually reduce the risk of heart attacks.
Should my children be tested for Lipoprotein(a) if my levels are high?
Because Lp(a) is a directly inherited genetic trait, first-degree relatives (children and siblings) of an individual with high levels should strongly consider being tested to establish their baseline risk early in life.
Why did my previous doctor never test me for Lipoprotein(a)?
Historically, Lp(a) testing was only recommended for very specific, extreme medical cases. However, recent advances in cardiology research have definitively proven its widespread danger, leading modern medical guidelines to now recommend universal screening for all adults.
Does high Lipoprotein(a) affect my heart valves?
Yes. In addition to clogging coronary arteries, Lp(a) specifically promotes heavy calcium buildup and inflammation on the aortic valve. This frequently leads to a condition called aortic stenosis, where the valve becomes stiff and eventually requires replacement.
If I have high Lp(a), do I need to take a daily aspirin?
Because Lp(a) promotes blood clotting, a low-dose daily aspirin is sometimes discussed. However, daily aspirin carries internal bleeding risks, so it is strictly prescribed on a case-by-case basis by an experienced cardiologist after reviewing your total clinical profile.
Expert Care
Hyderabad's leading Cardio & Neuro specialists.